

Metastasis after radical prostatectomy or external beam radiotherapy for patients with clinically localized prostate cancer: a comparison of clinical cohorts adjusted for case mix
- PMID: 20159826
- PMCID: PMC3731893
- DOI: 10.1200/JCO.2009.22.2265
Metastasis after radical prostatectomy or external beam radiotherapy for patients with clinically localized prostate cancer: a comparison of clinical cohorts adjusted for case mix
Abstract
Purpose: We assessed the effect of radical prostatectomy (RP) and external beam radiotherapy (EBRT) on distant metastases (DM) rates in patients with localized prostate cancer treated with RP or EBRT at a single specialized cancer center.
Patients and methods: Patients with clinical stages T1c-T3b prostate cancer were treated with intensity-modulated EBRT (> or = 81 Gy) or RP. Both cohorts included patients treated with salvage radiotherapy or androgen-deprivation therapy for biochemical failure. Salvage therapy for patients with RP was delivered a median of 13 months after biochemical failure compared with 69 months for EBRT patients. DM was compared controlling for patient age, clinical stage, serum prostate-specific antigen level, biopsy Gleason score, and year of treatment.
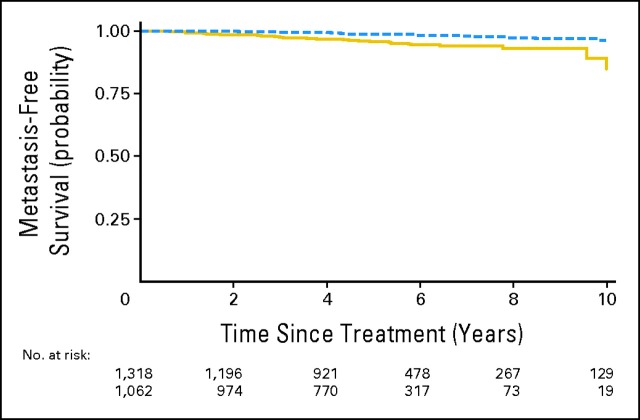
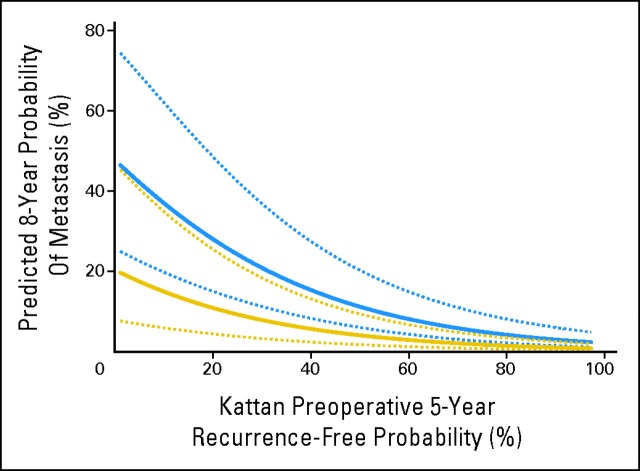
Results: The 8-year probability of freedom from metastatic progression was 97% for RP patients and 93% for EBRT patients. After adjustment for case mix, surgery was associated with a reduced risk of metastasis (hazard ratio, 0.35; 95% CI, 0.19 to 0.65; P < .001). Results were similar for prostate cancer-specific mortality (hazard ratio, 0.32; 95% CI, 0.13 to 0.80; P = .015). Rates of metastatic progression were similar for favorable-risk disease (1.9% difference in 8-year metastasis-free survival), somewhat reduced for intermediate-risk disease (3.3%), and more substantially reduced in unfavorable-risk disease (7.8% in 8-year metastatic progression).
Conclusion: Metastatic progression is infrequent in men with low-risk prostate cancer treated with either RP or EBRT. RP patients with higher-risk disease treated had a lower risk of metastatic progression and prostate cancer-specific death than EBRT patients. These results may be confounded by differences in the use and timing of salvage therapy.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Do not count out external-beam radiation therapy for high-risk prostate cancer.J Clin Oncol. 2010 Oct 1;28(28):e518-9; author reply e521-e522. doi: 10.1200/JCO.2010.28.9561. Epub 2010 Jul 26. J Clin Oncol. 2010. PMID: 20660824 No abstract available.
-
Pitfalls of retrospective and nonrandomized comparison of treatment modalities.J Clin Oncol. 2010 Oct 1;28(28):e520; author reply e521-e522. doi: 10.1200/JCO.2010.29.5352. Epub 2010 Jul 26. J Clin Oncol. 2010. PMID: 20660831 No abstract available.
References
-
- Bill-Axelson A, Holmberg L, Ruutu M, et al. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med. 2005;352:1977–1984. - PubMed
-
- Vickers AJ, Bianco FJ, Serio AM, et al. The surgical learning curve for prostate cancer control after radical prostatectomy. J Natl Cancer Inst. 2007;99:1171–1177. - PubMed
-
- Zelefsky MJ, Chan H, Hunt M, et al. Long-term outcome of high dose intensity modulated radiation therapy for patients with clinically localized prostate cancer. J Urol. 2006;176:1415–1419. - PubMed
-
- Cahlon O, Zelefsky MJ, Shippy A, et al. Ultra-high dose (86.4 Gy) IMRT for localized prostate cancer: Toxicity and biochemical outcomes. Int J Radiat Oncol Biol Phys. 2008;71:330–337. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
