

Evaluation of standard chemotherapy in the guinea pig model of tuberculosis
- PMID: 20160055
- PMCID: PMC2863665
- DOI: 10.1128/AAC.01521-09
Evaluation of standard chemotherapy in the guinea pig model of tuberculosis
Abstract
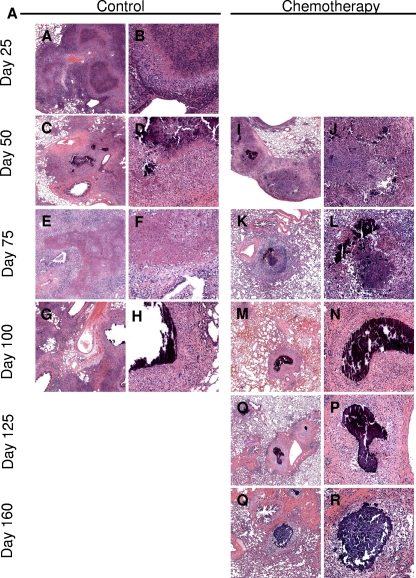
The purpose of this study was 2-fold. First, we evaluated standard chemotherapy in the guinea pig model of tuberculosis to determine if this animal species could productively be used for this purpose. Second, given the similarities of the pathology of disease in guinea pigs and humans, we wished to evaluate additional parameters, including magnetic resonance imaging, microscopy, and cytokine expression and lymphocyte phenotypes, in response to an infection treated with drug therapy. This study shows that conventional rifampin-isoniazid-pyrazinamide chemotherapy significantly decreased the numbers of the highly virulent Erdman K01 strain of Mycobacterium tuberculosis, with most of the bacilli being eliminated in a month. Despite this result, bacteria could still be detected in the lungs and other tissues for at least another 3 to 4 months. Resolution of the nonnecrotic granulomas in the lungs and lymph nodes could be clearly visualized by magnetic resonance imaging at the macroscopic level. Microscopically, the majority of the pulmonary and extrapulmonary inflammation resolved spontaneously, leaving residual lesions composed of dystrophic calcification and fibrosis marking the site of necrosis of the primary lesion. Residual calcified lesions, which were also associated with pulmonary lymphangitis, contained acid-fast bacilli even following aggressive chemotherapy. The presence of intact extracellular bacilli within these lesions suggests that these could serve as the primary sites of disease reactivation. The chemotherapy reduced the level of T-cell influx into infected tissues and was accompanied by a large and sustained increase in TH1 cytokine expression. Chemotherapy also prevented the emergence in lung tissues of high levels of interleukin-10 and Foxp3-positive cells, known markers of regulatory T cells.
Figures









Comment in
-
Activity of pyrazinamide in the guinea pig model of tuberculosis.Antimicrob Agents Chemother. 2010 Dec;54(12):5420. doi: 10.1128/AAC.00928-10. Antimicrob Agents Chemother. 2010. PMID: 21075978 Free PMC article. No abstract available.
References
-
- Aziz, M. A., A. Wright, A. Laszlo, A. De Muynck, F. Portaels, A. Van Deun, C. Wells, P. Nunn, L. Blanc, and M. Raviglione. 2006. Epidemiology of antituberculosis drug resistance (the Global Project on Anti-Tuberculosis Drug Resistance Surveillance): an updated analysis. Lancet 368:2142-2154. - PubMed
-
- Basaraba, R. J. 2008. Experimental tuberculosis: the role of comparative pathology in the discovery of improved tuberculosis treatment strategies. Tuberculosis (Edinb.) 88(Suppl. 1):S35-S47. - PubMed
-
- Basaraba, R. J., D. D. Dailey, C. T. McFarland, C. A. Shanley, E. E. Smith, D. N. McMurray, and I. M. Orme. 2006. Lymphadenitis as a major element of disease in the guinea pig model of tuberculosis. Tuberculosis (Edinb.) 86:386-394. - PubMed
-
- Basaraba, R. J., A. A. Izzo, L. Brandt, and I. M. Orme. 2006. Decreased survival of guinea pigs infected with Mycobacterium tuberculosis after multiple BCG vaccinations. Vaccine 24:280-286. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
