

Diverse patterns of T-cell response against multiple newly identified human Y chromosome-encoded minor histocompatibility epitopes
- PMID: 20160060
- PMCID: PMC2834217
- DOI: 10.1158/1078-0432.CCR-09-2701
Diverse patterns of T-cell response against multiple newly identified human Y chromosome-encoded minor histocompatibility epitopes
Abstract
Purpose: Donor T cells respond to minor histocompatibility antigens (mHA), resulting in both graft-versus-host disease and graft versus leukemia after allogeneic hematopoietic stem cell transplantation. Because relatively few mHAs are known, we developed a new approach to predict and subsequently validate candidate mHA.
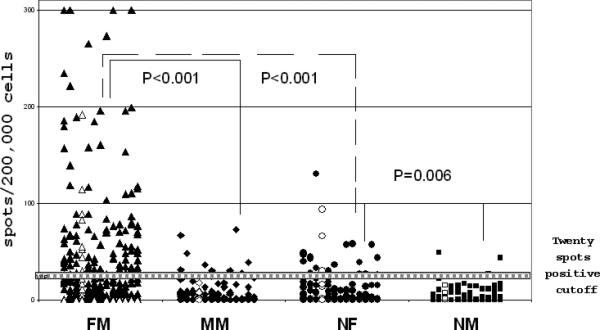
Experimental design: We developed an algorithm based on genetic disparities between Y chromosome-encoded and X chromosome-encoded proteins and known requirements for binding to HLA class I molecules to predict Y chromosome-derived, HLA A*0201-restricted peptides (HY) and ranked peptides based on potential immunogenicity. We evaluated T-cell responses to 41 candidate peptides in 28 male recipients with female donors (FM), 22 male recipients with male donors (MM), and 26 normal individuals. All patients and donors were HLA A*0201 positive.
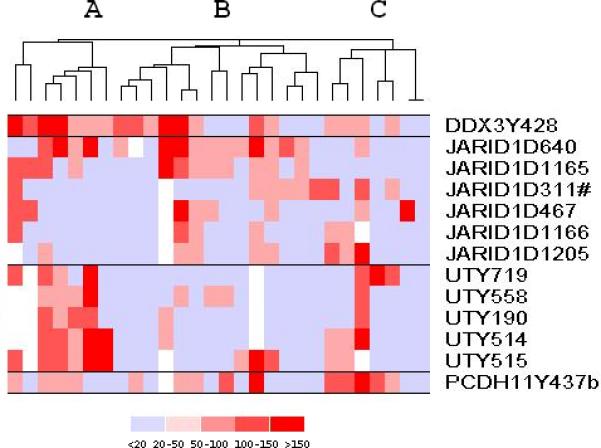
Results: Thirteen peptides derived from five proteins elicited significantly greater T-cell responses in FM patients compared with MM patients and in normal females compared with normal males. Six peptides were more immunogenic than the only previously known HLA A*0201-restricted Y-encoded mHA. Twenty-seven of 28 FM patients responded to at least one HY peptide, but despite a common Y chromosome mismatch and expression of HLA A*0201, each patient responded to a unique set of peptides.
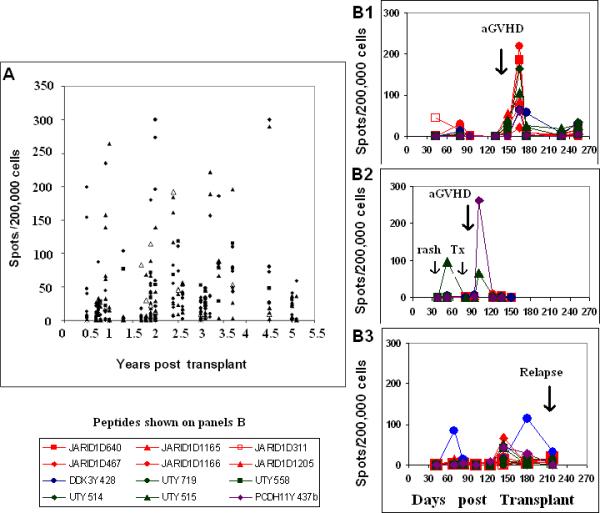
Conclusions: Novel HLA A*0201-restricted HY epitopes can be predicted and validated in patients after allogeneic hematopoietic stem cell transplantation. Highly diverse patterns of T-cell response against these epitopes have been identified. Prospective monitoring of responses to large panels of immunogenic peptides can facilitate the identification of clinically relevant targets of graft-versus-host disease and graft versus leukemia.
Figures

Similar articles
-
Common minor histocompatibility antigen discovery based upon patient clinical outcomes and genomic data.PLoS One. 2011;6(8):e23217. doi: 10.1371/journal.pone.0023217. Epub 2011 Aug 9. PLoS One. 2011. PMID: 21858034 Free PMC article.
-
Multicenter analyses demonstrate significant clinical effects of minor histocompatibility antigens on GvHD and GvL after HLA-matched related and unrelated hematopoietic stem cell transplantation.Biol Blood Marrow Transplant. 2013 Aug;19(8):1244-53. doi: 10.1016/j.bbmt.2013.06.001. Epub 2013 Jun 10. Biol Blood Marrow Transplant. 2013. PMID: 23756210
-
Optimized Whole Genome Association Scanning for Discovery of HLA Class I-Restricted Minor Histocompatibility Antigens.Front Immunol. 2020 Apr 17;11:659. doi: 10.3389/fimmu.2020.00659. eCollection 2020. Front Immunol. 2020. PMID: 32362897 Free PMC article.
-
Minor histocompatibility antigens to predict, monitor or manipulate GvL and GvHD after allogeneic hematopoietic cell transplantation.Best Pract Res Clin Haematol. 2024 Jun;37(2):101555. doi: 10.1016/j.beha.2024.101555. Epub 2024 May 15. Best Pract Res Clin Haematol. 2024. PMID: 39098803 Review.
-
Non-myeloablative transplants for malignant disease.Hematology Am Soc Hematol Educ Program. 2001:375-91. doi: 10.1182/asheducation-2001.1.375. Hematology Am Soc Hematol Educ Program. 2001. PMID: 11722994 Review.
Cited by
-
Determining the Quantitative Principles of T Cell Response to Antigenic Disparity in Stem Cell Transplantation.Front Immunol. 2018 Oct 11;9:2284. doi: 10.3389/fimmu.2018.02284. eCollection 2018. Front Immunol. 2018. PMID: 30364159 Free PMC article. Review.
-
Chromosome Y-encoded antigens associate with acute graft-versus-host disease in sex-mismatched stem cell transplant.Blood Adv. 2018 Oct 9;2(19):2419-2429. doi: 10.1182/bloodadvances.2018019513. Blood Adv. 2018. PMID: 30262602 Free PMC article.
-
Exploiting T cells specific for human minor histocompatibility antigens for therapy of leukemia.Immunol Cell Biol. 2011 Mar;89(3):396-407. doi: 10.1038/icb.2010.124. Epub 2011 Feb 8. Immunol Cell Biol. 2011. PMID: 21301477 Free PMC article. Review.
-
Genome-wide minor histocompatibility matching as related to the risk of graft-versus-host disease.Blood. 2017 Feb 9;129(6):791-798. doi: 10.1182/blood-2016-09-737700. Epub 2016 Nov 21. Blood. 2017. PMID: 27872059 Free PMC article.
-
Minor histocompatibility antigens and the maternal immune response to the fetus during pregnancy.Am J Reprod Immunol. 2013 Apr;69(4):304-14. doi: 10.1111/aji.12075. Epub 2013 Feb 8. Am J Reprod Immunol. 2013. PMID: 23398025 Free PMC article. Review.
References
-
- Bleakley M, Riddell SR. Molecules and mechanisms of the graft versus leukemia effect. Nat Rev Cancer. 2004;4:371–80. - PubMed
-
- Shlomchik WD. Graft versus Host disease. Nat Rev Immunol. 2007;7:340–52. - PubMed
-
- Mullally A, Ritz J. Beyond HLA: the significance of genomic variation for allogeneic hematopoietic stem cell transplantation. Blood. 2007;109:1355–62. - PubMed
-
- Goulmy E. Minor histocompatibility antigens: from transplantation problems to therapy of cancer. Hum Immunol. 2006;67:433–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
