

The utility of non-axial treatment beam orientations for lower lobe lung cancers
- PMID: 20160689
- PMCID: PMC5719787
- DOI: 10.1120/jacmp.v11i1.3010
The utility of non-axial treatment beam orientations for lower lobe lung cancers
Abstract
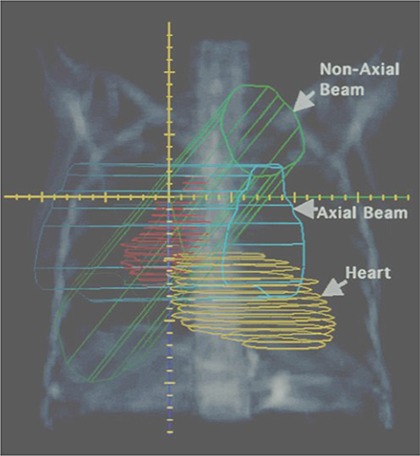
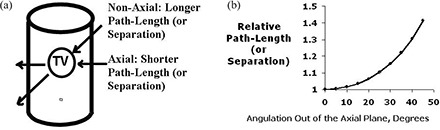
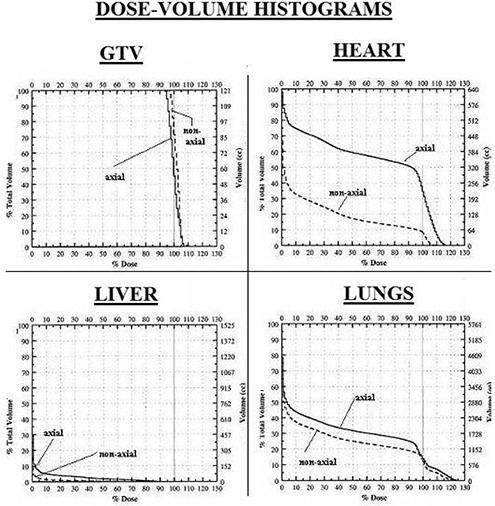
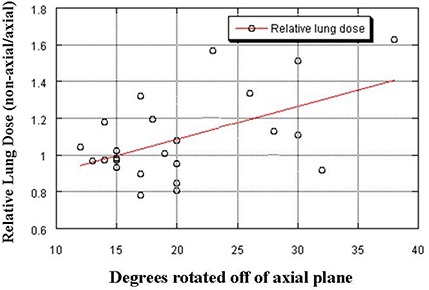
Traditional treatment beams for non-small-cell lung cancer are limited to the axial plane. For many tumor geometries, non-axial orientations appear to reduce the dose to normal tissues (e.g. heart, liver). We hypothesize that non-axial beams provide a significant reduction in incidental irradiation of the heart and liver, while maintaining adequate target coverage. CT scans of twenty-four patients with lower lobe lung cancers were studied. For each patient, an opposed oblique axial beam pair and a competing non-axial opposed oblique pair were generated, both off-cord. The competing plans delivered comparable doses/margins to the GTV. DVHs and integral doses were computed for all structures of interest for the two competing plans. The integral dose was compared for axial and non-axial beams for each contoured organ using a paired t-test. Dose to the heart was significantly lower for the non-axial plans ( p = .0001). For 20/24 patients, the integral heart dose was reduced by using non-axial beams. In those patients with tumors located in the inferior right lower lobe, a lower dose to the liver was achieved when non-axial beams were used. There were no meaningful differences in dose to the GTV, lungs, or skin between axial and non-axial beams. Non-axial beams can reduce the dose to the heart and liver in patients with lower lobe lung cancers. Non-axial beams may be clinically beneficial in these patients and should be considered as an option during planning.
Figures
Similar articles
-
Accumulation of the delivered dose based on cone-beam CT and deformable image registration for non-small cell lung cancer treated with hypofractionated radiotherapy.BMC Cancer. 2020 Nov 16;20(1):1112. doi: 10.1186/s12885-020-07617-3. BMC Cancer. 2020. PMID: 33198676 Free PMC article.
-
4π noncoplanar stereotactic body radiation therapy for centrally located or larger lung tumors.Int J Radiat Oncol Biol Phys. 2013 Jul 1;86(3):407-13. doi: 10.1016/j.ijrobp.2013.02.002. Epub 2013 Mar 21. Int J Radiat Oncol Biol Phys. 2013. PMID: 23523322
-
Feasibility of sparing lung and other thoracic structures with intensity-modulated radiotherapy for non-small-cell lung cancer.Int J Radiat Oncol Biol Phys. 2004 Mar 15;58(4):1268-79. doi: 10.1016/j.ijrobp.2003.09.085. Int J Radiat Oncol Biol Phys. 2004. PMID: 15001272
-
Intermediate Megavoltage Photon Beams for Improved Lung Cancer Treatments.PLoS One. 2015 Dec 16;10(12):e0145117. doi: 10.1371/journal.pone.0145117. eCollection 2015. PLoS One. 2015. PMID: 26672752 Free PMC article.
-
Intensity-modulated radiotherapy for locally advanced non-small-cell lung cancer: a dose-escalation planning study.Int J Radiat Oncol Biol Phys. 2011 May 1;80(1):306-13. doi: 10.1016/j.ijrobp.2010.06.025. Epub 2010 Oct 1. Int J Radiat Oncol Biol Phys. 2011. PMID: 20888706
References
-
- Gyenes G, Rutqvist L, Liedberg A, Fornander T. Long‐term cardiac morbidity and mortality in a randomized trial of pre‐ and postoperative radiation therapy versus surgery alone in primary breast cancer. Radiother Oncol. 1998;48(2):185–90. - PubMed
-
- Stewart JR, Fajard LF, Gillette SM, Constine LS. Radiation injury to the heart. Int J Radiat Oncol Biol Phys. 1995;31(5):1205–11. - PubMed
-
- Heidenreich PA, Hancock SL, Lee BK, Mariscal CS, Schnittger I. Asymptomatic cardiac disease following mediastinal irradiation. J Am Coll Cardiol. 2003;42(4):743–49. - PubMed
-
- Eriksson F, Gagliardi G, Liedberg A, et al. Long‐term cardiac mortality following radiation therapy for Hodgkin's disease: analysis with the relative seriality model. Radiother Oncol. 2000;55(2):153–62. - PubMed
-
- Glanzmann C, Kaufmann P, Jenni R, Hess OM, Huguenin P. Cardiac risk after mediastinal irradiation for Hodgkin's disease. Radiother Oncol. 1998;46(1):51–62. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
