

Winter Depression: Integrating mood, circadian rhythms, and the sleep/wake and light/dark cycles into a bio-psycho-social-environmental model
- PMID: 20160896
- PMCID: PMC2768314
- DOI: 10.1016/j.jsmc.2009.02.003
Winter Depression: Integrating mood, circadian rhythms, and the sleep/wake and light/dark cycles into a bio-psycho-social-environmental model
Abstract
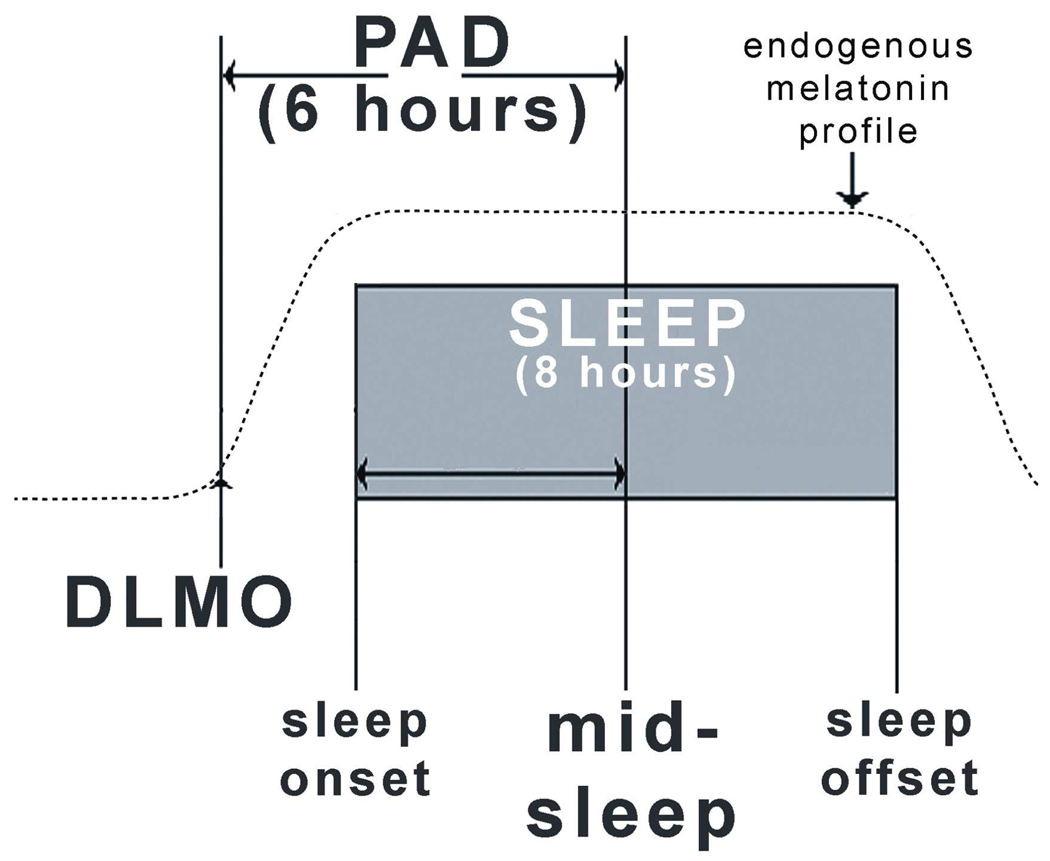
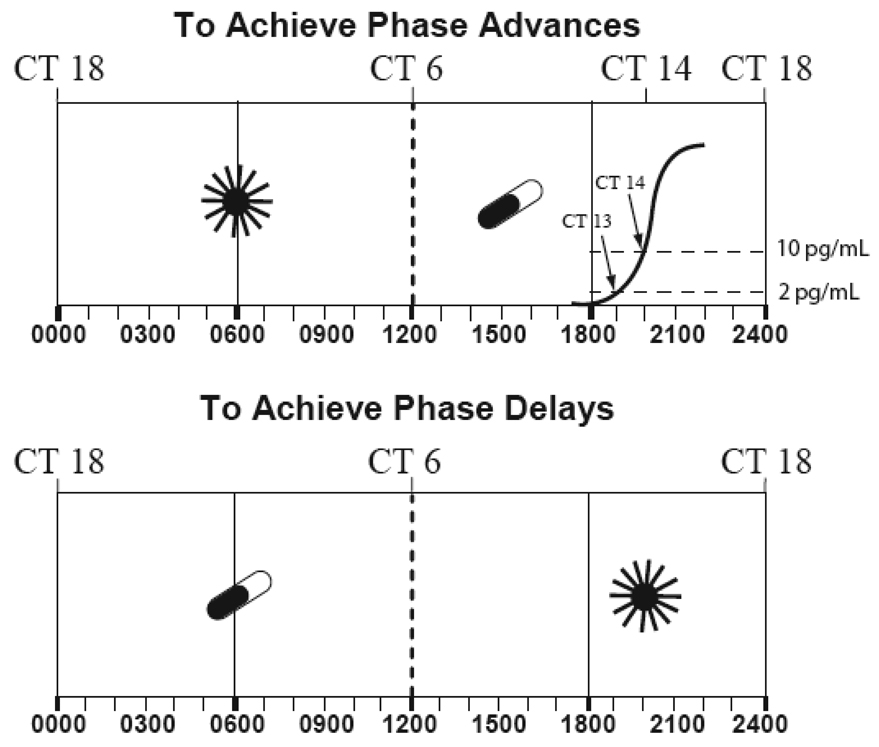
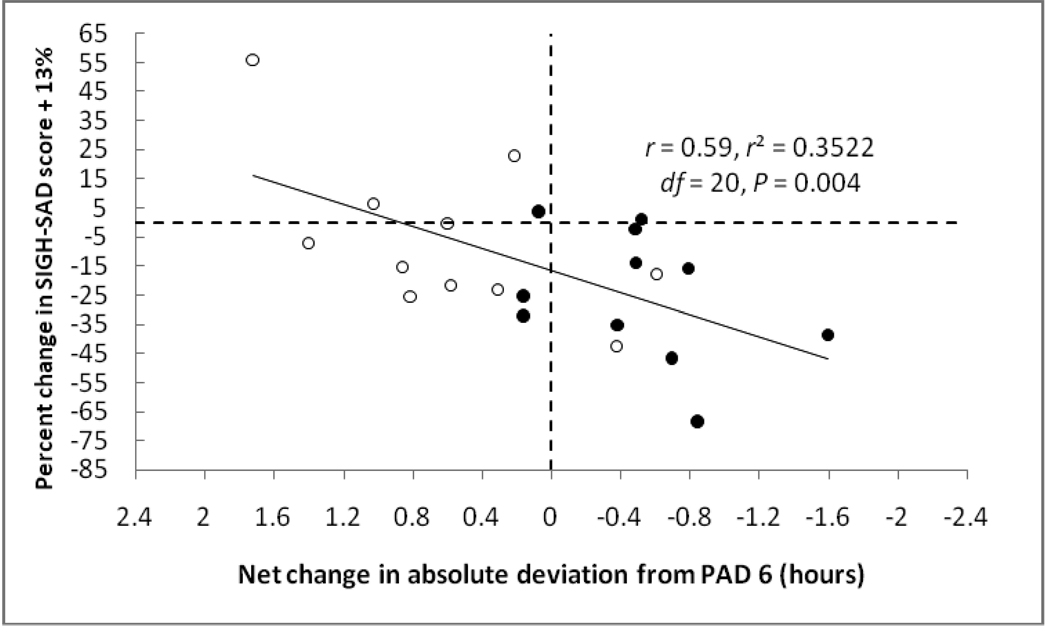
The phase shift hypothesis (PSH) states that most patients with SAD become depressed in the winter because of a delay in circadian rhythms with respect to the sleep/wake cycle: According to the PSH, these patients should preferentially respond to the antidepressant effects of bright light exposure when it is scheduled in the morning so as to provide a corrective phase advance and restore optimum alignment between the circadian rhythms tightly coupled to the endogenous circadian pacemaker and those rhythms that are related to the sleep/wake cycle. Recent support for the PSH has come from studies in which symptom severity was shown to correlate with the degree of circadian misalignment: it appears that a subgroup of patients are phase advanced, not phase delayed; however, the phase-delayed type is predominant in SAD and perhaps in other disorders as well, such as non-seasonal unipolar depression. It is expected that during the next few years the PSH will be tested in these and other conditions, particularly since healthy subjects appear to have more severe symptoms of sub-clinical dysphoria correlating with phase-delayed circadian misalignment; critically important will be the undertaking of treatment trials to investigate the therapeutic efficacy of morning bright light or afternoon/evening low-dose melatonin in these disorders in which symptoms are more severe as the dim light melatonin onset (DLMO) is delayed with respect to the sleep/wake cycle (non-restorative sleep should also be evaluated, as well as bipolar disorder). The possibility that some individuals (and disorders) will be of the phase-advanced type should be considered, taking into account that the correct timing of phase-resetting agents for them will be bright light scheduled in the evening and/or low-dose melatonin taken in the morning. While sleep researchers and clinicians are accustomed to phase-typing patients with circadian-rhythm sleep disorders according to the timing of sleep, phase typing based on the DLMO with respect to the sleep/wake cycle may lead to quite different recommendations for the optimal scheduling of phase-resetting agents, particularly for the above disorders and conditions.
Figures
Similar articles
-
Circadian misalignment in mood disturbances.Curr Psychiatry Rep. 2009 Dec;11(6):459-65. doi: 10.1007/s11920-009-0070-5. Curr Psychiatry Rep. 2009. PMID: 19909668 Review.
-
The phase shift hypothesis for the circadian component of winter depression.Dialogues Clin Neurosci. 2007;9(3):291-300. doi: 10.31887/DCNS.2007.9.3/alewy. Dialogues Clin Neurosci. 2007. PMID: 17969866 Free PMC article. Review.
-
Phase advancing human circadian rhythms with morning bright light, afternoon melatonin, and gradually shifted sleep: can we reduce morning bright-light duration?Sleep Med. 2015 Feb;16(2):288-97. doi: 10.1016/j.sleep.2014.12.004. Epub 2014 Dec 18. Sleep Med. 2015. PMID: 25620199 Free PMC article.
-
Circadian rhythm sleep disorders: pathophysiology and potential approaches to management.CNS Drugs. 2001;15(4):311-28. doi: 10.2165/00023210-200115040-00005. CNS Drugs. 2001. PMID: 11463135 Review.
-
Human seasonal and circadian studies in Antarctica (Halley, 75°S).Gen Comp Endocrinol. 2018 Mar 1;258:250-258. doi: 10.1016/j.ygcen.2017.05.010. Epub 2017 May 17. Gen Comp Endocrinol. 2018. PMID: 28526480
Cited by
-
Circadian misalignment in mood disturbances.Curr Psychiatry Rep. 2009 Dec;11(6):459-65. doi: 10.1007/s11920-009-0070-5. Curr Psychiatry Rep. 2009. PMID: 19909668 Review.
-
Sleep in seasonal affective disorder.Curr Opin Psychol. 2020 Aug;34:7-11. doi: 10.1016/j.copsyc.2019.08.023. Epub 2019 Aug 26. Curr Opin Psychol. 2020. PMID: 31536962 Free PMC article. Review.
-
Timing of sleep and its relationship with the endogenous melatonin rhythm.Front Neurol. 2010 Nov 1;1:137. doi: 10.3389/fneur.2010.00137. eCollection 2010. Front Neurol. 2010. PMID: 21188265 Free PMC article.
-
Characteristics of Mild Cognitive Impairment in Northern Japanese Community-Dwellers from the ORANGE Registry.J Clin Med. 2019 Nov 10;8(11):1937. doi: 10.3390/jcm8111937. J Clin Med. 2019. PMID: 31717664 Free PMC article.
-
Delayed sleep phase syndrome is related to seasonal affective disorder.J Affect Disord. 2011 Oct;133(3):573-9. doi: 10.1016/j.jad.2011.04.046. Epub 2011 May 20. J Affect Disord. 2011. PMID: 21601293 Free PMC article.
References
-
- Rosen LN, Rosenthal NE. Seasonal variations in mood and behavior in the general population: a factor-analytic approach. Psychiatry Research. 1991;38:271–283. - PubMed
-
- Rosenthal NE, Sack DA, Gillin JC, et al. Seasonal affective disorder: a description of the syndrome and preliminary findings with light therapy. Archives of General Psychiatry. 1984;41:72–80. - PubMed
-
- Kasper S, Wehr TA, Bartko JJ, Gaist PA, Rosenthal NE. Epidemiological findings of seasonal changes in mood and behavior. Archives of General Psychiatry. 1989;46:823–833. - PubMed
-
- Rosenthal NE, Carpenter CJ, James SP, Parry BL, Rogers S, Wehr TA. Seasonal affective disorder in children and adolescents. American Journal of Psychiatry. 1986;143(3):356–358. - PubMed
-
- Swedo SE, Pleeter JD, Richter DM, et al. Rates of seasonal affective disorder in children and adolescents. American Journal of Psychiatry. 1995;152:1016–1019. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
