

doi: 10.1097/CPM.0b013e3181c849fe.
Multidisciplinary Evaluation of Patients With Suspected Lung Cancer
Affiliations
- PMID: 20161592
- PMCID: PMC2808634
- DOI: 10.1097/CPM.0b013e3181c849fe
Item in Clipboard
Multidisciplinary Evaluation of Patients With Suspected Lung Cancer
Clin Pulm Med.
.
Abstract
Lung cancer diagnosis and treatment has evolved to require the input and expertise of multiple diverse medical and surgical specialties. The approach to lung cancer patients requires the adherence to a few principles that include thorough use of staging modalities to assure the proper treatment for each patient, and an understanding of the limitations and advantages of each of these modalities. Evidence is continuing to emerge that supports the notion that diagnostic workup and treatment of lung cancer patients is best done within the context of a multidisciplinary team devoted to this purpose.
Figures
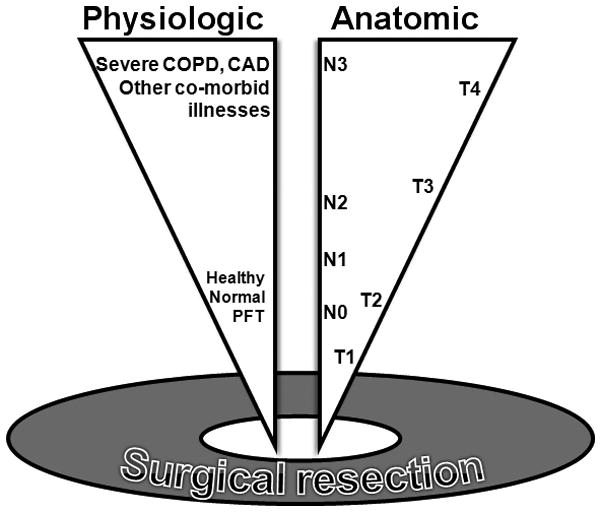
Patients undergoing lung cancer surgery bring with them to the OR a certain burden that can be measured in both anatomic (tumor) and physiologic (co-morbid) terms. Only so much of each can be sustained for a patient to successfully withstand lobectomy or greater operations (chest wall resection, pneumonectomy). Considering patients for surgery requires an accurate knowledge of not just the tumor stage (as determined by parameters of tumor “T”, nodal “N”, and metastatic “M” extent), but also of the patients “physiologic stage”. Patients with more extensive disease can undergo surgery if they are otherwise in good physiologic condition. Likewise, patients with more co-morbidity can withstand more limited operations, but (for example) not pneumonectomy or chest wall resection.
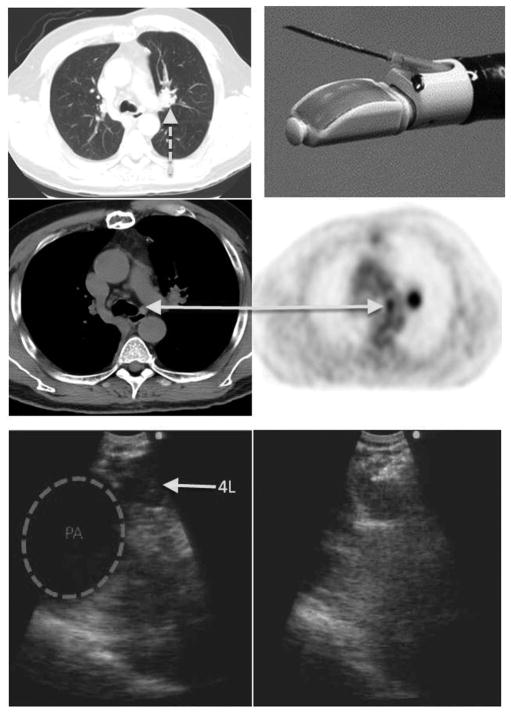
CT scan showing the presence of a left hilar nodule (Dashed arrow, top left). Combined CT-PET scan shows uptake in the left hilar mass, as well as a small left paratracheal lymph node (Station 4L. Middle row arrow). Endobronchial ultrasound (EBUS) shows the 4L node adjacent to the pulmonary artery (bottom left). Color doppler allows the bronchoscopist to confirm the presence of vessels. EBUS guided needle aspiration of the 4L node demonstrated malignant involvement of the N2 nodes, providing a stage and a diagnosis in one procedure (Bottom right panel shows the needle in the plane of the ultrasound, entering the node). The top right panel shows the linear array ultrasound at the end of the bronchoscope with the needle protruding from the working channel.
Similar articles
-
Navigating Diagnostic and Treatment Decisions in Non-Small Cell Lung Cancer: Expert Commentary on the Multidisciplinary Team Approach.Oncologist. 2021 Feb;26(2):e306-e315. doi: 10.1002/onco.13586. Epub 2020 Nov 21. Oncologist. 2021. PMID: 33145902 Free PMC article. Review.
-
Accuracy of lung cancer staging in the multidisciplinary team setting.Transl Lung Cancer Res. 2020 Aug;9(4):1654-1666. doi: 10.21037/tlcr.2019.11.28. Transl Lung Cancer Res. 2020. PMID: 32953539 Free PMC article. Review.
-
The Role of Multidisciplinary Care Planning on Survival, Care Quality, and Satisfaction for Patients with Lung Cancer [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2020 Feb. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2020 Feb. PMID: 39471259 Free Books & Documents. Review.
-
Clinical and organizational factors in the initial evaluation of patients with lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines.Chest. 2013 May;143(5 Suppl):e121S-e141S. doi: 10.1378/chest.12-2352. Chest. 2013. PMID: 23649435 Free PMC article.
-
[Chinese expert consensus on multidisciplinary discussion of interstitial lung disease].Zhonghua Jie He He Hu Xi Za Zhi. 2023 Dec 12;46(12):1176-1188. doi: 10.3760/cma.j.cn112147-20230726-00030. Zhonghua Jie He He Hu Xi Za Zhi. 2023. PMID: 37989522 Chinese.
Cited by
-
Surgical consensus for screening, diagnosis, staging, multimodal management and surveillance of early-stage resectable non-small cell lung cancer (NSCLC) in Malaysia.Transl Lung Cancer Res. 2025 Jul 31;14(7):2403-2426. doi: 10.21037/tlcr-2025-296. Epub 2025 Jul 28. Transl Lung Cancer Res. 2025. PMID: 40799423 Free PMC article. Review.
-
Integration of tobacco cessation services into multidisciplinary lung cancer care: rationale, state of the art, and future directions.Transl Lung Cancer Res. 2015 Aug;4(4):339-52. doi: 10.3978/j.issn.2218-6751.2015.07.15. Transl Lung Cancer Res. 2015. PMID: 26380175 Free PMC article. Review.
-
Diagnosis of lung cancer by flexible fiberoptic bronchoscopy: a descriptive study.Rom J Morphol Embryol. 2022 Apr-Jun;63(2):369-381. doi: 10.47162/RJME.63.2.08. Rom J Morphol Embryol. 2022. PMID: 36374142 Free PMC article.
References
-
- Alberts WM. Introduction: Diagnosis and Management of Lung Cancer*. Chest. 2007;132:20S–22S. - PubMed
-
- Ettinger D, Johnson B. Update: NCCN small cell and non-small cell lung cancer Clinical Practice Guidelines. J Natl Compr Canc Netw. 2005;3 (Suppl 1):S17–21. - PubMed
-
- Gabel M, Hilton NE, Nathanson SD. Multidisciplinary breast cancer clinics. Do they work? Cancer. 1997;79:2380–2384. - PubMed
-
- Newman EA, Guest AB, Helvie MA, et al. Changes in surgical management resulting from case review at a breast cancer multidisciplinary tumor board. Cancer. 2006;107:2346–2351. - PubMed
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009 caac.20006. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources