

Risk of subsequent fracture and mortality within 5 years after a non-vertebral fracture
- PMID: 20162259
- PMCID: PMC2974915
- DOI: 10.1007/s00198-010-1178-5
Risk of subsequent fracture and mortality within 5 years after a non-vertebral fracture
Abstract
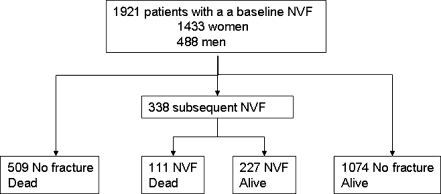
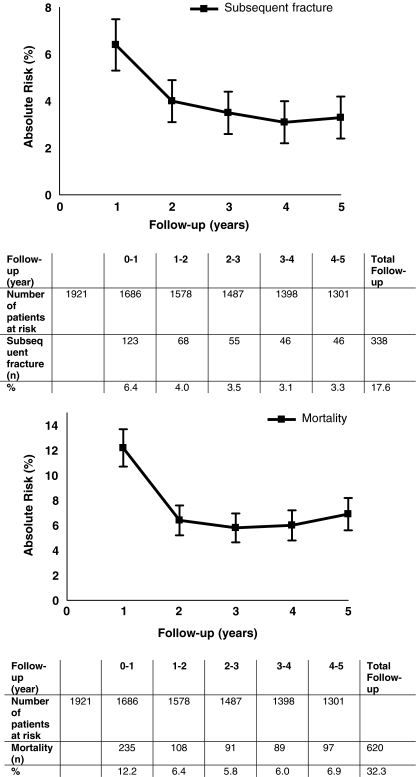
Summary: The absolute 5-year risk of subsequent non-vertebral fractures (NVFs) in 1,921 patients presenting with a NVF was 17.6% and of mortality was 32.3%. These risks were highest within the first year, indicating the need to study which reversible factors can be targeted to immediately minimise subsequent fracture risk and mortality.
Introduction: NVFs are the most frequent clinical fractures in patients presenting at the emergency unit because of a clinical fracture. The aim of the study was to determine the 5-year absolute risk (AR) of subsequent NVF and mortality in patients at the time they present with a NVF.
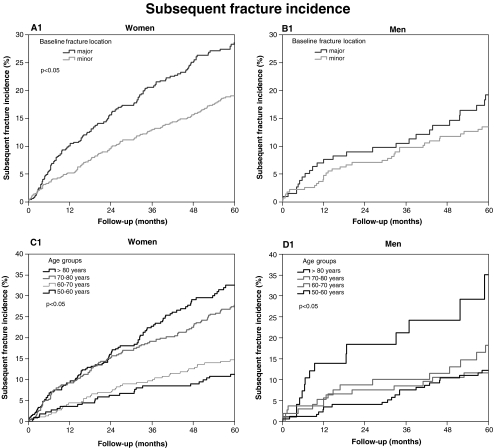
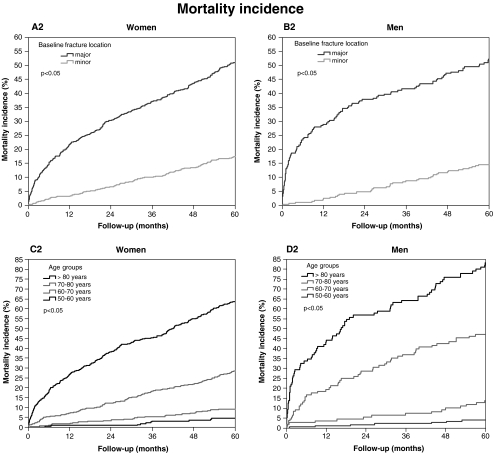
Methods: Between 1999 and 2001, 1,921 consecutive patients 50+ years from a level 1 trauma centre were included. All NVFs were confirmed on radiograph reports, and mortality was checked in the national obituary database. Available potential risk factors for a subsequent NVF and mortality (age, sex and baseline fracture location: major-hip, pelvis, multiple ribs, proximal tibia/humerus and distal femur; minor-all others) were expressed as hazard ratios (HR) with 95% confidence intervals (CI) using multivariable Cox regression analysis.
Results: The AR for a subsequent NVF was 17.6% and was related to age (HR per decade, 1.44; 95%CI, 1.29-1.60). The AR for mortality was 32.3% and was related to age (HR per decade, 2.59; 95%CI, 2.37-2.84), male sex (HR, 1.74; 95%CI, 1.44-2.10), major fracture at baseline (HR, 5.56; 95%CI, 3.48-8.88; not constant over time) and subsequent fracture (HR, 1.65; 95%CI, 1.33-2.05). The highest risks were found within the first year (NVFs, 6.4%; mortality, 12.2%) and were related to age and, in addition, to baseline fracture location for mortality.
Conclusions: Within 5 years after an initial NVF, nearly one in five patients sustained a subsequent NVF and one in three died. One third of subsequent NVFs and mortality occurred within 1 year, indicating the need to study which reversible factors can be targeted to immediately prevent subsequent fractures and mortality.
Figures
References
-
- Kanis JA, Johnell O, De Laet C, Johansson H, Oden A, Delmas P, Eisman J, Fujiwara S, Garnero P, Kroger H, McCloskey EV, Mellstrom D, Melton LJ, Pols H, Reeve J, Silman A, Tenenhouse A. A meta-analysis of previous fracture and subsequent fracture risk. Bone. 2004;35:375–382. doi: 10.1016/j.bone.2004.03.024. - DOI - PubMed
-
- van Geel TA, van Helden S, Geusens PP, Winkens B, Dinant GJ. Clinical subsequent fractures cluster in time after first fractures. Ann Rheum Dis. 2009;68:101–104. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
