

Cause of death in patients with lower-risk myelodysplastic syndrome
- PMID: 20162709
- PMCID: PMC3753205
- DOI: 10.1002/cncr.24984
Cause of death in patients with lower-risk myelodysplastic syndrome
Abstract
Background: The authors have recently shown that a majority of patients with myelodysplastic syndrome (MDS) classified by the International Prognostic Scoring System as lower risk die without transformation to acute myelogenous leukemia (AML). The cause of death (COD) of these patients is not well understood. Identifying the COD could help to guide early therapy decisions.
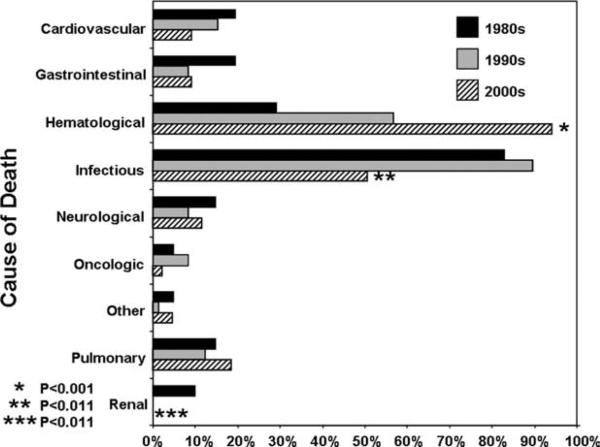
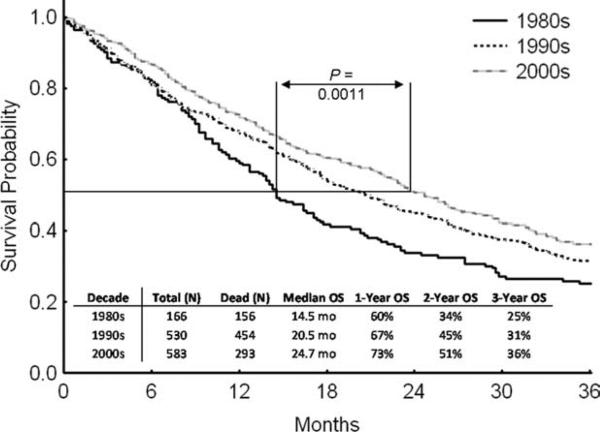
Methods: The authors retrospectively analyzed the COD in a cohort of 273 deceased patients with lower-risk MDS according to the International Prognostic Scoring System at presentation to The University of Texas M. D. Anderson Cancer Center from 1980 to 2004. MDS-related death was defined as infection, bleeding, transformation to AML, or disease progression. Remaining CODs were classified as non-MDS-related.
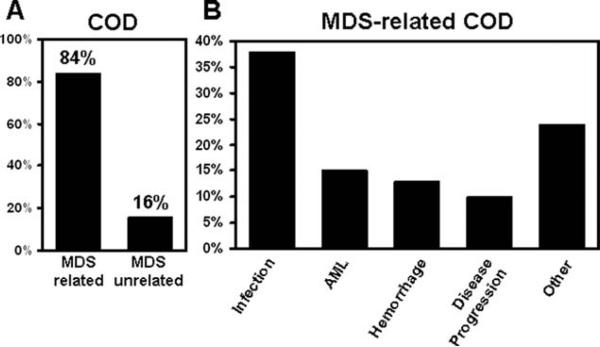
Results: Median age at presentation was 66 years (range, 19-88 years). Overall median survival was 59 weeks (range, 1-831 weeks). All French-American-British leukemia classification subgroups were represented. The percentage of International Prognostic Scoring System low and intermediate-1 groups were 21% and 79%, respectively. The most common cytogenetic abnormality (9%) was del(5q). Patients received supportive care only. The COD was identified as MDS-related in 230 of 273 (84%) patients. The most common disease-related CODs were infection (38%), transformation to AML (15%), and hemorrhage (13%). The most frequent non-disease-related COD was cardiovascular events (19 of 43 patients).
Conclusions: The majority of patients with low- or intermediate-1 risk MDS will die because of causes related to their underlying disease. Although these results need to be validated in different populations, early therapeutic intervention could be considered in the management of these patients to improve survival.
(c) 2010 American Cancer Society.
Figures
Comment in
-
Should patients with low-risk myelodysplastic syndrome be treated earlier in the course of their disease?Curr Hematol Malig Rep. 2011 Mar;6(1):1-2. doi: 10.1007/s11899-010-0072-8. Curr Hematol Malig Rep. 2011. PMID: 21161616 No abstract available.
References
-
- Greenberg P, Cox C, LeBeau MM, Fenaux P, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood. 1997;89:2079–2088. - PubMed
-
- Rollison DE, Howlader N, Smith MT, et al. Epidemiology of myelodysplastic syndromes and chronic myeloproliferative disorders in the United States, 2001-2004, using data from the NAACCR and SEER programs. Blood. 2008;112:45–52. - PubMed
-
- Garcia-Manero G, Shan J, Faderl S, et al. A prognostic score for patients with lower risk myelodysplastic syndrome. Leukemia. 2008;22:538–543. - PubMed
-
- Ma X, Does M, Raza A, Mayne ST. Myelodysplastic syndromes: incidence and survival in the United States. Cancer. 2007;109:1536–1542. - PubMed
-
- Kantarjian H, Issa JP, Rosenfeld CS, et al. Decitabine improves patient outcomes in myelodysplastic syndromes: results of a phase III randomized study. Cancer. 2006;106:1794–1803. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
