

Effects of intracranial trochlear neurectomy on the structure of the primate superior oblique muscle
- PMID: 20164458
- PMCID: PMC2904006
- DOI: 10.1167/iovs.09-5120
Effects of intracranial trochlear neurectomy on the structure of the primate superior oblique muscle
Abstract
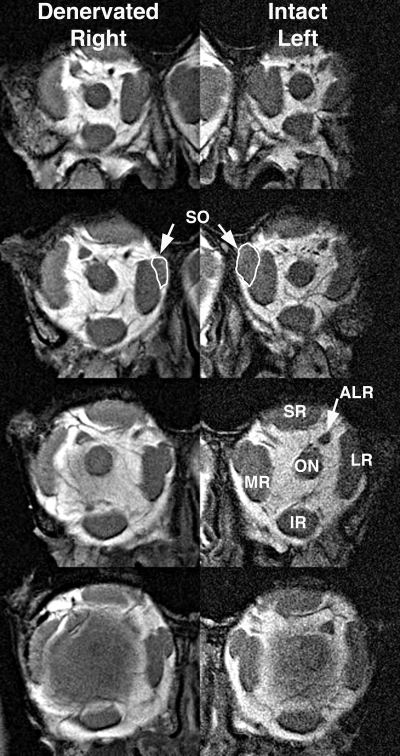
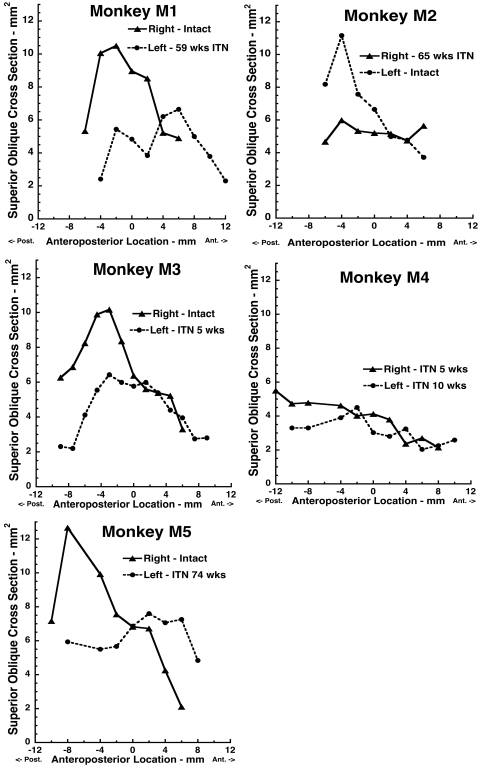
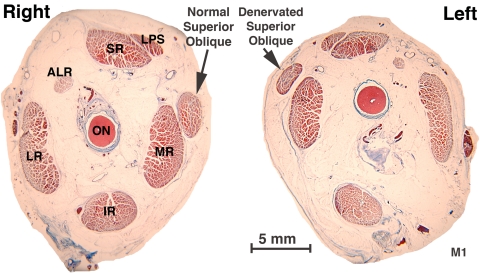
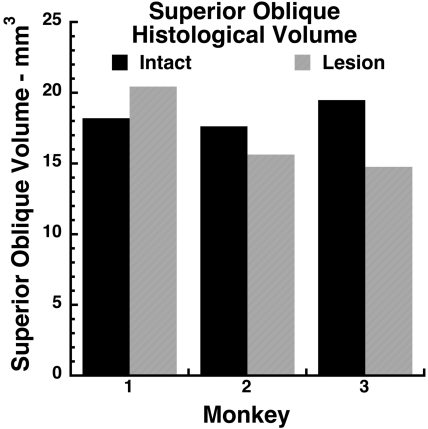
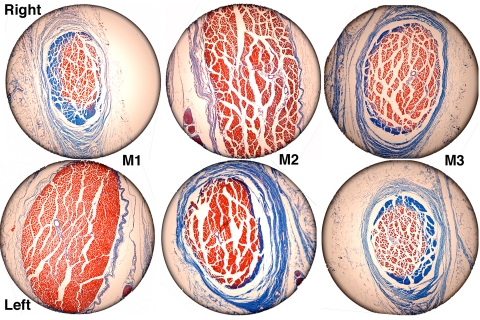
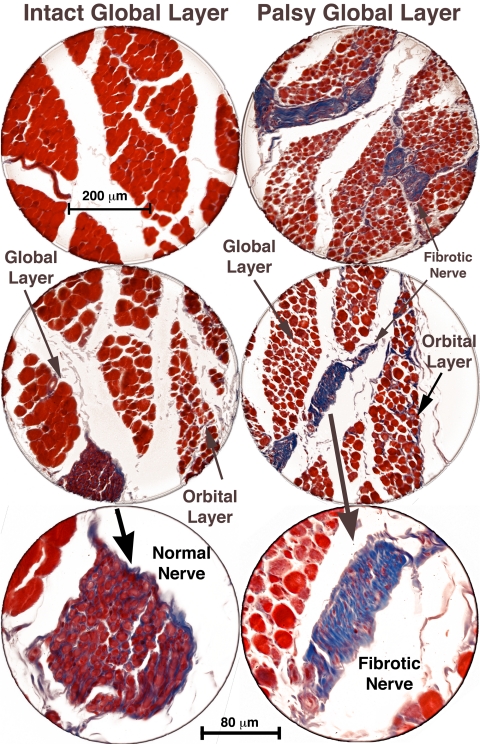
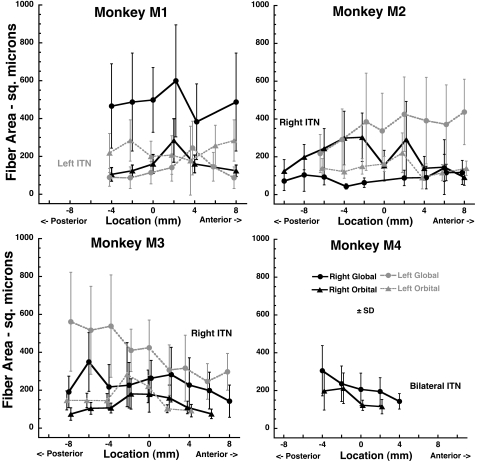
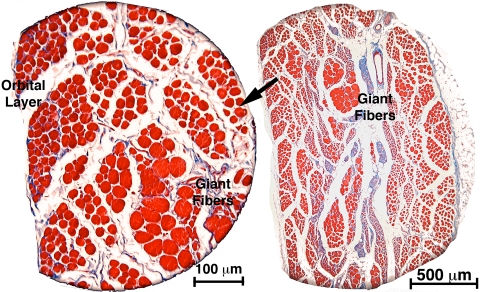
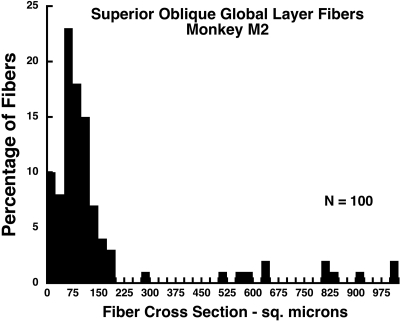
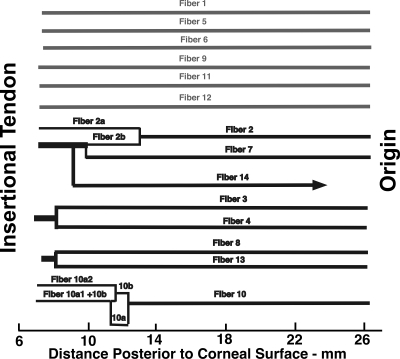
PURPOSE. Although cyclovertical strabismus in humans is frequently attributed to superior oblique (SO) palsy, anatomic effects of SO denervation have not been studied. Magnetic resonance imaging (MRI) and orbital histology was used to study the effects of acute trochlear (CN4) denervation on the monkey SO. METHODS. Five juvenile macaque monkeys were perfused with formalin for 5 weeks: 15 months after unilateral or bilateral 10-mm intracranial trochlear neurectomy. Denervated and fellow orbits were imaged by MRI, embedded whole in paraffin, serially sectioned at 10-mum thickness, and stained with Masson trichrome. Whole muscle and individual fiber cross sections were quantified in SO muscles throughout the orbit and traced larger fibers in one specimen where they were present. RESULTS. MRI demonstrated marked reduction in midorbital cross section in denervated SO muscles, with anterior shift of SO mass preserving overall volume. Muscle fibers exhibited variable atrophy along their lengths. Denervated orbital layer (OL) fiber cross sections were slightly but significantly reduced from control at most anteroposterior locations, but this reduction was much more profound in global layer (GL) fibers. Intraorbital and intramuscular CN4 were uniformly fibrotic. In one animal, there were scattered clusters of markedly hypertrophic GL fibers that exhibited only sparse myomyous junctions only anteriorly. CONCLUSIONS. CN4 denervation produces predominantly SO GL atrophy with relative OL sparing. Overall midorbital SO atrophy was evident by MRI as early as 5 weeks after denervation, as denervated SO volume shifted anteriorly. Occasional GL fiber hypertrophy suggests that at least some SO fibers extend essentially the full muscle length after trochlear neurectomy.
Figures
References
-
- Bielschowsky A. Lectures on motor anomalies. XI. Etiology, prognosis, and treatment of ocular paralyses. Am J Ophthalmol 1939;22:723–734
-
- von Noorden GK, Murray E, Wong SY. Superior oblique paralysis: a review of 270 cases. Arch Ophthalmol 1986;104:1771–1776 - PubMed
-
- Adler FE. Physiologic factors in differential diagnosis of paralysis of superior rectus and superior oblique muscles. Arch Ophthalmol 1946;36:661–673 - PubMed
-
- Scott WE, Kraft SP. Classification and treatment of superior oblique palsies: II. Bilateral superior oblique palsies. In: Caldwell D. ed. Pediatric Ophthalmology and Strabismus: Transactions of the New Orleans Academy of Ophthalmology New York: Raven Press; 1986:265–291 - PubMed
-
- Scott WE, Parks MM. Differential diagnosis of vertical muscle palsies. In: von Noorden GK. ed. Symposium on Strabismus: Transactions of the New Orleans Academy of Ophthalmology.St. Louis: Mosby; 1978:118–134
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
