

Intraspinal anomalies in scoliosis: An MRI analysis of 177 consecutive scoliosis patients
- PMID: 20165678
- PMCID: PMC2822421
- DOI: 10.4103/0019-5413.58607
Intraspinal anomalies in scoliosis: An MRI analysis of 177 consecutive scoliosis patients
Abstract
Background: The association of intraspinal neural anomalies with scoliosis is known for more than six decades. However, there are no studies documenting the incidence of association of intraspinal anomalies in scoliotic patients in the Indian population. The guide lines to obtain an magnetic resonance imaging (MRI) scan to rule out neuro-axial abnormalities in presumed adolescent idiopathic scoliosis are also not clear. We conducted a prospective study (a) to document and analyze the incidence and types of intraspinal anomalies in different types of scoliosis in Indian patients. (b) to identify clinico-radiological 'indicators' that best predict the findings of neuro-axial abnormalities in patients with presumed adolescent idiopathic scoliosis, which will alert the physician to the possible presence of intraspinal anomalies and optimize the use of MRI in this sub group of patients.
Materials and methods: The data from 177 consecutive scoliotic patients aged less than 21 years were analyzed. Patients were categorized into three groups; Group A - congenital scoliosis (n=60), group B -presumed idiopathic scoliosis (n=94) and group C - scoliosis secondary to neurofibromatosis, neuromuscular and connective tissue disorders (n=23). The presence and type of anomaly in the MRI was correlated to patient symptoms, clinical signs and curve characteristics.
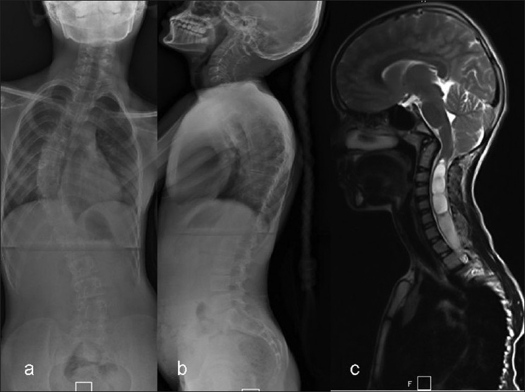
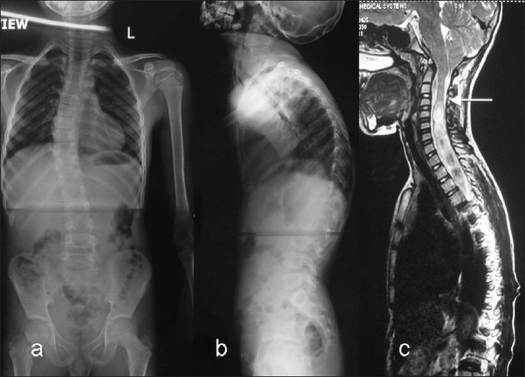
Results: The incidence of intraspinal anomalies in congenital scoliosis was 35% (21/60), with tethered cord due to filum terminale being the commonest anomaly (10/21). Patients with multiple vertebral anomalies had the highest incidence (48%) of neural anomalies and isolated hemi vertebrae had none. In presumed 'idiopathic' scoliosis patients the incidence was higher (16%) than previously reported. Arnold Chiari-I malformation (AC-I) with syringomyelia was the most common neural anomaly (9/15) and the incidence was higher in the presence of neurological findings (100%), apical kyphosis (66.6%) and early onset scoliosis. Isolated lumbar curves had no anomalies. In group-C, incidence was 22% and most of the anomalies were in curves with connective tissue disorders.
Conclusion: The high incidence of intraspinal anomalies in presumed idiopathic scoliosis in our study group emphasizes the need for detailed examination for subtle neurological signs that accompany neuro-axial anomalies. Preoperative MRI screening is recommended in patients with presumed 'idiopathic' scoliosis who present at young age, with neurological findings and in curves with apical thoracic kyphosis.
Keywords: Intraspinal anomalies; MRI scan; neuro-axial anomalies; scoliosis.
Conflict of interest statement
Figures
Similar articles
-
Vertebral and Intraspinal Anomalies in Indian Population with Congenital Scoliosis: A Study of 119 Consecutive Patients.Asian Spine J. 2016 Apr;10(2):276-81. doi: 10.4184/asj.2016.10.2.276. Epub 2016 Apr 15. Asian Spine J. 2016. PMID: 27114768 Free PMC article.
-
The prevalence of intraspinal anomalies in infantile and juvenile patients with "presumed idiopathic" scoliosis: a MRI-based analysis of 504 patients.BMC Musculoskelet Disord. 2016 Apr 27;17:189. doi: 10.1186/s12891-016-1026-7. BMC Musculoskelet Disord. 2016. PMID: 27121616 Free PMC article.
-
Intraspinal anomalies in infantile idiopathic scoliosis: prevalence and role of magnetic resonance imaging.Spine (Phila Pa 1976). 2009 May 20;34(12):E434-8. doi: 10.1097/BRS.0b013e3181a2b49f. Spine (Phila Pa 1976). 2009. PMID: 19454995
-
Prevalence and risk factors for neural axis anomalies in idiopathic scoliosis: a systematic review.Spine J. 2018 Jul;18(7):1261-1271. doi: 10.1016/j.spinee.2018.02.013. Epub 2018 Feb 14. Spine J. 2018. PMID: 29454133
-
Intraspinal anomalies in early-onset idiopathic scoliosis.Bone Joint J. 2017 Jun;99-B(6):829-833. doi: 10.1302/0301-620X.99B6.BJJ-2016-1159.R1. Bone Joint J. 2017. PMID: 28566405 Review.
Cited by
-
Vertebral, rib, and intraspinal anomalies in congenital scoliosis: a study on 202 Caucasians.Eur Spine J. 2015 Jul;24(7):1510-21. doi: 10.1007/s00586-015-3833-1. Epub 2015 Mar 3. Eur Spine J. 2015. PMID: 25733202
-
Patterns of congenital bony spinal deformity and associated neural anomalies on X-ray and magnetic resonance imaging.J Child Orthop. 2016 Aug;10(4):343-52. doi: 10.1007/s11832-016-0752-6. Epub 2016 Jun 23. J Child Orthop. 2016. PMID: 27339475 Free PMC article.
-
Vertebral and Intraspinal Anomalies in Indian Population with Congenital Scoliosis: A Study of 119 Consecutive Patients.Asian Spine J. 2016 Apr;10(2):276-81. doi: 10.4184/asj.2016.10.2.276. Epub 2016 Apr 15. Asian Spine J. 2016. PMID: 27114768 Free PMC article.
-
Simultaneous Surgical Treatment of Congenital Spinal Deformity Associated with Intraspinal Anomalies.Asian Spine J. 2018 Jun;12(3):466-475. doi: 10.4184/asj.2018.12.3.466. Epub 2018 Jun 4. Asian Spine J. 2018. PMID: 29879774 Free PMC article.
-
Incidence of intraspinal abnormalities in congenital scoliosis: a systematic review and meta-analysis.J Orthop Surg Res. 2020 Oct 21;15(1):485. doi: 10.1186/s13018-020-02015-8. J Orthop Surg Res. 2020. PMID: 33087139 Free PMC article.
References
-
- McMaster MJ. Occult intraspinal anomalies and congenital scoliosis. J Bone Joint Surg Am. 1984;66:588–601. - PubMed
-
- Noordeen MH, Taylor BA, Edgar MA. Syringomyelia: A potential risk factor in scoliosis surgery. Spine. 1994;19:1406–9. - PubMed
-
- Ozerdemoglu RA, Denis F, Transfeldt EE. Scoliosis associated with syringomyelia: Clinical and radiologic correlation. Spine. 2003;28:1410–7. - PubMed
-
- MacEwen GD, Bunnell WP, Sriram K. Acute neurological complications in the treatment of scoliosis: A report of the Scoliosis Research Society. J Bone Joint Surg Am. 1975;57:404–8. - PubMed
-
- Peer S, Krismer M, Judmaier W, Kerber W. The value of MRI in the preoperative assessment of scoliosis. Orthopade. 1994;23:318–22. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials