

Greater cardiac response of colloid than saline fluid loading in septic and non-septic critically ill patients with clinical hypovolaemia
- PMID: 20165941
- PMCID: PMC2837190
- DOI: 10.1007/s00134-010-1776-x
Greater cardiac response of colloid than saline fluid loading in septic and non-septic critically ill patients with clinical hypovolaemia
Abstract
Background and objective: The haemodynamics of crystalloid and colloid fluid loading may depend on underlying disease, i.e. sepsis versus non-sepsis.
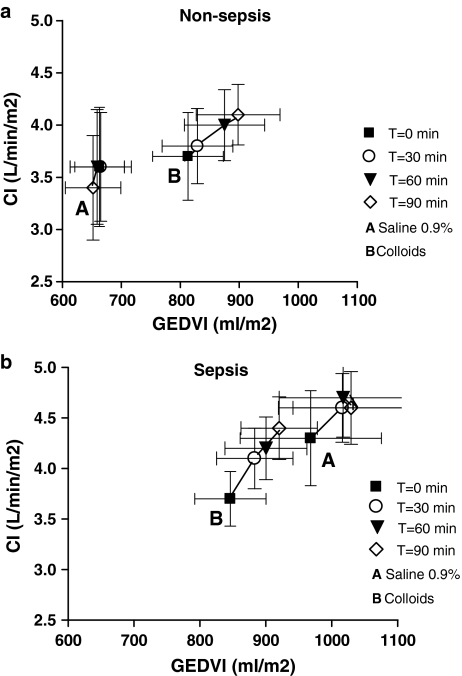
Design and setting: A single-centre, single-blinded, randomized clinical trial was carried out on 24 critically ill sepsis and 24 non-sepsis patients with clinical hypovolaemia, assigned to loading with normal saline, gelatin 4%, hydroxyethyl starch 6% or albumin 5% in a 90-min (delta) central venous pressure (CVP)-guided fluid loading protocol. Transpulmonary thermodilution was done each 30 min, yielding, among others, global end-diastolic volume and cardiac indices (GEDVI, CI).
Results: Sepsis patients had hyperdynamic hypotension in spite of myocardial depression and dilatation, and greater inotropic/vasopressor requirements than non-sepsis patients. Independent of underlying disease, CVP and GEDVI increased more after colloid than saline loading (P < 0.018), so that CI increased by about 2% after saline and 12% after colloid loading (P = 0.029). The increase in preload-recruitable stroke work was also greater with colloids and did not differ among conditions.
Conclusion: Fluid loading with colloids results in a greater linear increase in cardiac filling, output and stroke work than does saline loading, in both septic and non-septic clinical hypovolaemia, in spite of myocardial depression and presumably increased vasopermeability potentially decreasing the effects of colloid fluid loading in the former.
Figures
References
-
- Boldt J. Volume replacement in the surgical patient-does the type of solution make a difference? Br J Anaesth. 2000;84:783–793. - PubMed
-
- Perel P, Roberts J (2007) Colloids versus crystalloids for fluid resuscitation in critically ill patients. Cochrane Database Syst Rev (4):CD000567 - PubMed
-
- Dubois M-J, Orellana-Jimenez C, Mélot C, De Backer D, Berré J, Leeman M, Brimioulle S, Appoloni O, Creteur J, Vincent JL. Albumin administration improves organ function in critically ill hypoalbuminemic patients: a prospective, randomized, controlled pilot study. Crit Care Med. 2006;23:2336–2540. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
