

Increasing incidence of empyema complicating childhood community-acquired pneumonia in the United States
- PMID: 20166818
- PMCID: PMC4696869
- DOI: 10.1086/650573
Increasing incidence of empyema complicating childhood community-acquired pneumonia in the United States
Abstract
Background: The incidence of childhood pneumonia decreased following introduction of 7-valent pneumococcal conjugate vaccine (PCV7) in the United States. Recent regional reports suggest an increase in the incidence of childhood pneumonia complicated by empyema. We assessed whether early decreases in pneumonia hospitalization rates were sustained and trends in such hospitalizations complicated by empyema in United States children aged <5 years.
Methods: Nationwide Inpatient Sample and Census data were used to calculate annual all-cause and pneumococcal pneumonia hospitalization rates for pre-PCV7 (1996-1999) and post-PCV7 years (2001-2007) and to analyze national trends in total and pathogen-specific pneumonia-associated empyema.
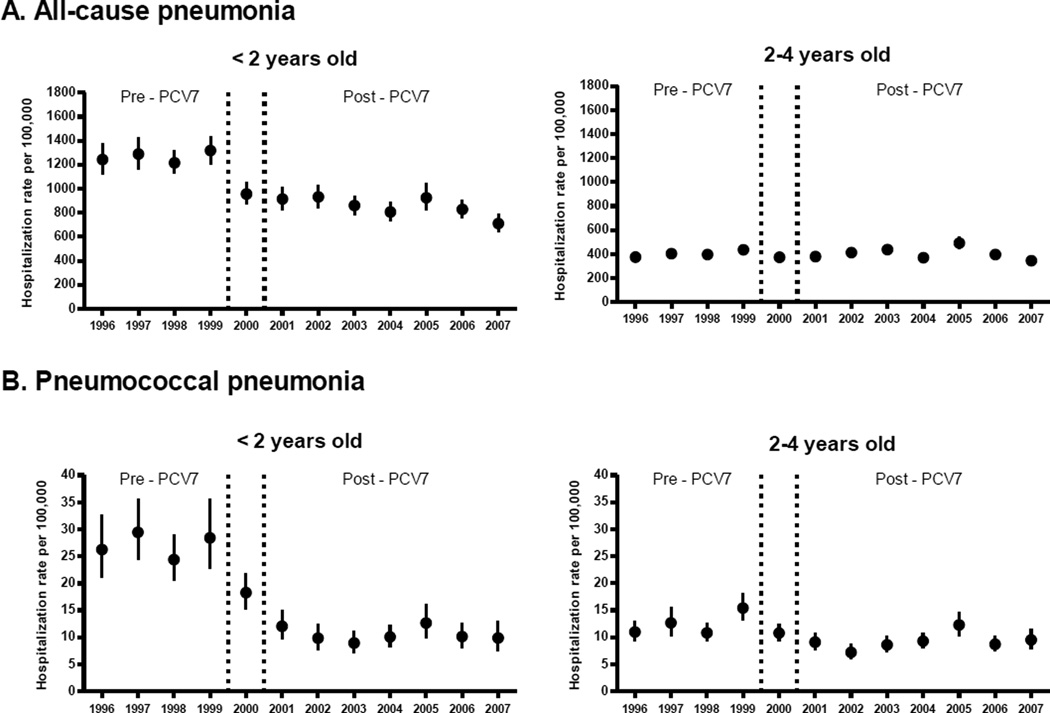
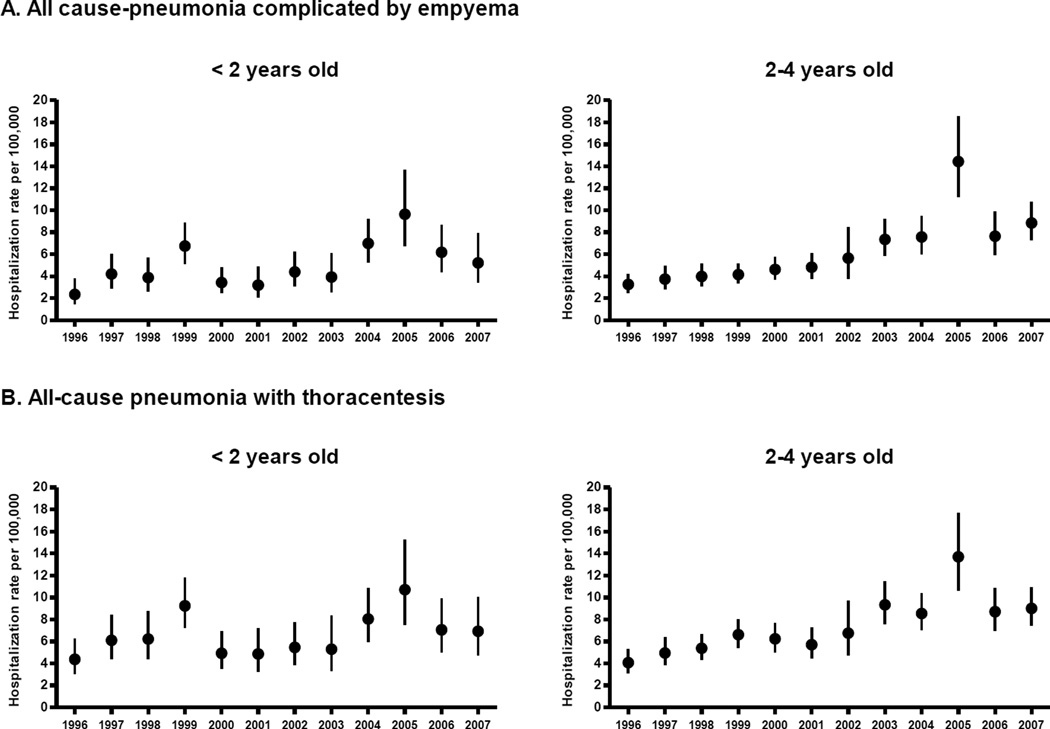
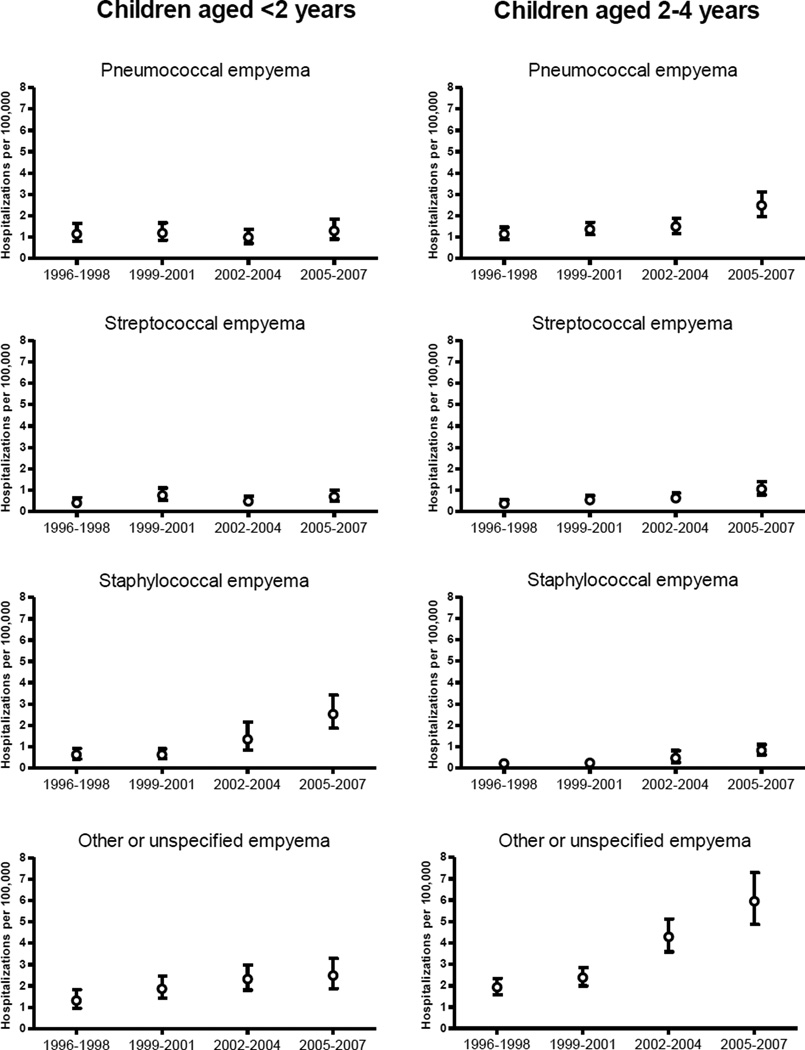
Results: Among children aged <2 years, all-cause pneumonia hospitalizations decreased 33% (95% confidence interval, 28%-37%) from 1267 cases per 100,000 children in pre-PCV7 years to 852 cases per 100,000 children in post-PCV7 years. Pneumococcal pneumonia hospitalization rates decreased 61% (95% confidence interval, 55%-67%) post-PCV7, compared with pre-PCV7 years. Pneumonia hospitalizations complicated by empyema increased 2.01-fold from 3.5 cases per 100,000 children in 1996-1998 to 7.0 cases per 100,000 children in 2005-2007. Rates of pneumococcal and streptococcal empyema remained stable, whereas rates of staphylococcal and other or unspecified empyema increased 4.08- and 1.89-fold, respectively. Among children aged 2-4 years, all-cause pneumonia rates remained stable, whereas pneumococcal pneumonia decreased by 26% (95% confidence interval, 16-34). Pneumonia complicated by empyema increased 2.81-fold from 3.7 cases per 100,000 children in 1996-1998 to 10.3 cases per 100,000 children in 2005-2007. In this age group, there were 2.17-, 2.80-, 3.76-, and 3.09-fold increases in rates of pneumococcal, streptococcal, staphylococcal, and other or unspecified empyema, respectively.
Conclusion: Decreases in childhood pneumonia hospitalization rates following PCV7 introduction were sustained. Although empyema complicated only a small fraction of pneumonia hospitalizations, its prevalence increased substantially. This increase was due to several pathogens and warrants continuing monitoring.
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
References
-
- Black S, Shinefield H, Fireman B, Lewis E, Ray P, Hansen JR. Efficacy, safety and immunogenicity of heptavalent pneumococcal conjugate vaccine in children. Pediatric Infectious Disease Journal. 2000;19:187–195. - PubMed
-
- Klugman KP, Madhi SA, Huebner RE, Kohberger R, Mbelle N, Pierce N. A trial of a 9-valent pneumococcal conjugate vaccine in children with and those without HIV infection. N Engl J Med. 2003;349(14):1341–1348. - PubMed
-
- Cutts FT, Zaman SM, Enwere G, et al. Efficacy of nine-valent pneumococcal conjugate vaccine against pneumonia and invasive pneumococcal disease in The Gambia: randomised, double-blind, placebo-controlled trial. Lancet. 2005;365(9465):1139–1146. - PubMed
-
- Lucero MG, Nohynek H, Williams G, et al. Efficacy of an 11-valent pneumococcal conjugate vaccine against radiologically confirmed pneumonia among children less than 2 years of age in the Philippines: a randomized, double-blind, placebo-controlled trial. Pediatr Infect Dis J. 2009 Jun;28(6):455–462. - PubMed
-
- Mulholland K. Childhood pneumonia mortality--a permanent global emergency. Lancet. 2007 Jul 21;370(9583):285–289. - PubMed
