

Center variation and outcomes associated with delayed sternal closure after stage 1 palliation for hypoplastic left heart syndrome
- PMID: 20167337
- PMCID: PMC2907662
- DOI: 10.1016/j.jtcvs.2009.11.029
Center variation and outcomes associated with delayed sternal closure after stage 1 palliation for hypoplastic left heart syndrome
Abstract
Objective: There is debate whether primary or delayed sternal closure is the best strategy after stage 1 palliation for hypoplastic left heart syndrome. We describe center variation in delayed sternal closure after stage 1 palliation and associated outcomes.
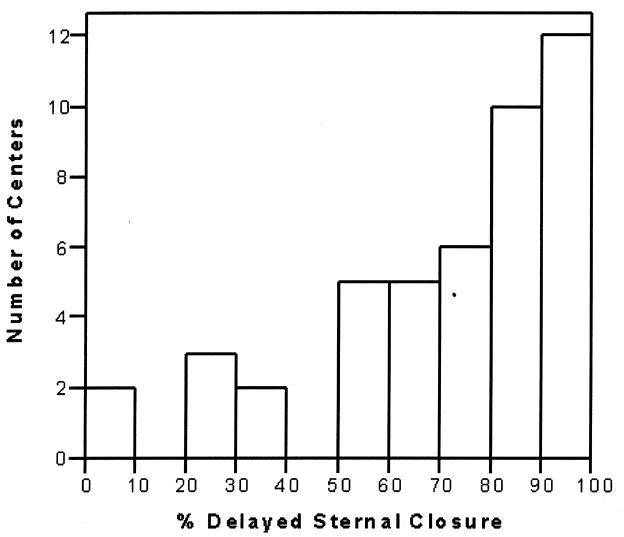
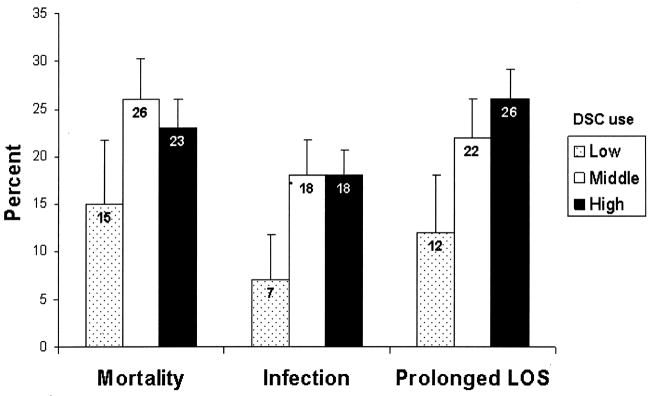
Methods: Society of Thoracic Surgeons Congenital Database participants performing stage 1 palliation for hypoplastic left heart syndrome from 2000 to 2007 were included. We examined center variation in delayed sternal closure and compared in-hospital mortality, prolonged length of stay (length of stay > 6 weeks), and postoperative infection in centers with low (< or = 25% of cases), middle (26%-74% of cases), and high (> or = 75% of cases) delayed sternal closure use, adjusting for patient and center factors.
Results: There were 1283 patients (45 centers) included. Median age at surgery was 6 days (interquartile range, 4-9 days), and median weight at surgery was 3.2 kg (interquartile range, 2.8-3.5 kg); 59% were male. Delayed sternal closure was used in 74% of cases (range, 3%-100% of cases/center). In centers with high (n = 23) and middle (n = 17) versus low (n = 5) delayed sternal closure use, there was a greater proportion of patients with prolonged length of stay and infection, and a trend toward increased in-hospital mortality in unadjusted analysis. In multivariable analysis, there was no difference in mortality. Centers with high and middle delayed sternal closure use had prolonged length of stay (odds ratio, 2.83; 95% confidence interval, 1.46-5.47; P = .002 and odds ratio, 2.23; confidence interval, 1.17-4.26; P = .02, respectively) and more infection (odds ratio, 2.34; confidence interval, 1.20-4.57; P = .01 and odds ratio, 2.37; confidence interval, 1.36-4.16; P = .003, respectively).
Conclusion: Use of delayed sternal closure after stage 1 palliation varies widely. These observational data suggest that more frequent use of delayed sternal closure is associated with longer length of stay and higher postoperative infection rates. Further evaluation of the risks and benefits of delayed sternal closure in the management of these complex infants is necessary.
2010 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Seghaye MC, Grabitz RG, Duchateau J, Busse S, Dabritz S, Koch D. Inflammatory reaction and capillary leak syndrome related to cardiopulmonary bypass in neonates undergoing cardiac operations. J Thorac Cardiovasc Surg. 1996;112:687–97. - PubMed
-
- McElhinney DB, Reddy VM, Parry AJ, Johnson L, Fineman JR, Hanley FL. Management and outcomes of delayed sternal closure after cardiac surgery in neonates and infants. Crit Care Med. 2000;28:1180–4. - PubMed
-
- Kay PH, Brass T, Lincoln C. The pathophysiology of atypical tamponade in infants undergoing cardiac surgery. Eur J Cardiothorac Surg. 1989;3:255–61. - PubMed
-
- Wernovsky G, Ghanayem N, Ohye RG, Bacha EA, Jacobs JP, Gaynor JW, et al. Hypoplastic left heart syndrome: consensus and controversies in 2007. Cardiol Young. 2007;17:S75–86. - PubMed
-
- Riphagen S, McDougall M, Tibby SM, Alphonso N, Anderson D, Austin C, et al. “Early” delayed sternal closure following pediatric cardiac surgery. Ann Thorac Surg. 2005;80:678–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
