

Avosentan for overt diabetic nephropathy
- PMID: 20167702
- PMCID: PMC2831858
- DOI: 10.1681/ASN.2009060593
Avosentan for overt diabetic nephropathy
Abstract
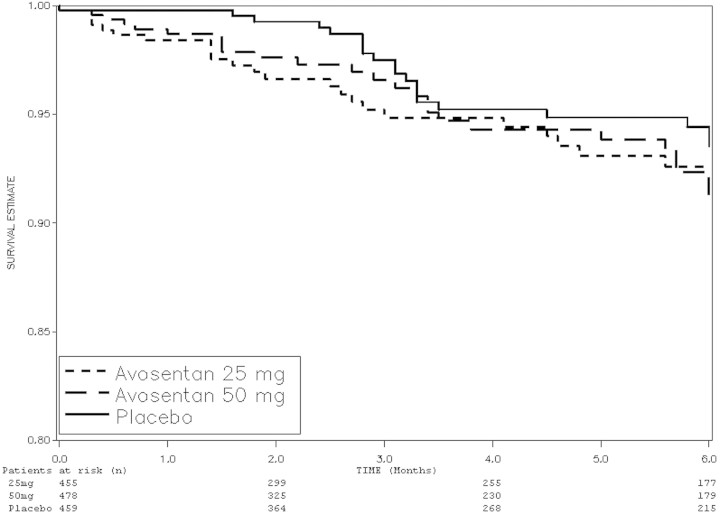
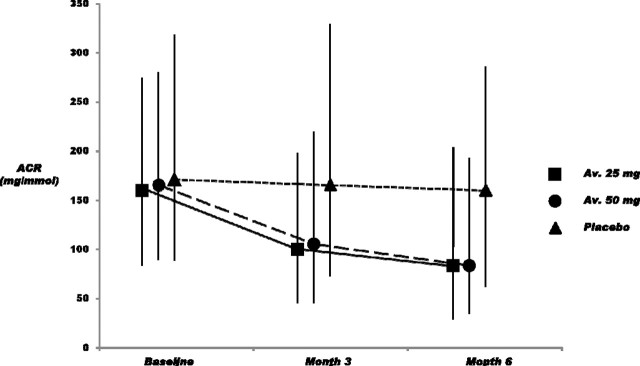
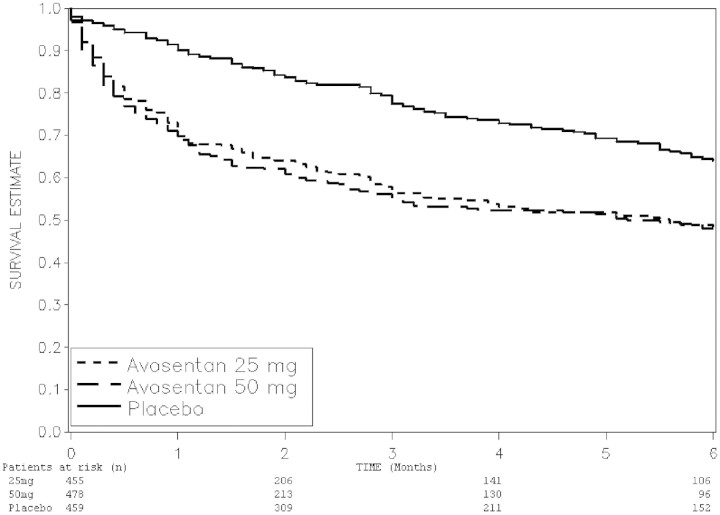
In the short term, the endothelin antagonist avosentan reduces proteinuria, but whether this translates to protection from progressive loss of renal function is unknown. We examined the effects of avosentan on progression of overt diabetic nephropathy in a multicenter, multinational, double-blind, placebo-controlled trial. We randomly assigned 1392 participants with type 2 diabetes to oral avosentan (25 or 50 mg) or placebo in addition to continued angiotensin-converting enzyme inhibition and/or angiotensin receptor blockade. The composite primary outcome was the time to doubling of serum creatinine, ESRD, or death. Secondary outcomes included changes in albumin-to-creatinine ratio (ACR) and cardiovascular outcomes. We terminated the trial prematurely after a median follow-up of 4 months (maximum 16 months) because of an excess of cardiovascular events with avosentan. We did not detect a difference in the frequency of the primary outcome between groups. Avosentan significantly reduced ACR: In patients who were treated with avosentan 25 mg/d, 50 mg/d, and placebo, the median reduction in ACR was 44.3, 49.3, and 9.7%, respectively. Adverse events led to discontinuation of trial medication significantly more often for avosentan than for placebo (19.6 and 18.2 versus 11.5% for placebo), dominated by fluid overload and congestive heart failure; death occurred in 21 (4.6%; P = 0.225), 17 (3.6%; P = 0.194), and 12 (2.6%), respectively. In conclusion, avosentan reduces albuminuria when added to standard treatment in people with type 2 diabetes and overt nephropathy but induces significant fluid overload and congestive heart failure.
Figures

Comment in
-
Endothelin receptor antagonists in proteinuric renal disease: every rose has its thorn.J Am Soc Nephrol. 2010 Mar;21(3):392-4. doi: 10.1681/ASN.2010010047. Epub 2010 Feb 4. J Am Soc Nephrol. 2010. PMID: 20133487 Free PMC article. No abstract available.
References
-
- Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH: Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345: 861–869, 2001 - PubMed
-
- Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB: Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 345: 851–860, 2001 - PubMed
-
- Jafar TH, Schmid CH, Landa M, Giatras I, Toto R, Remuzzi G: Angiotensin-converting enzyme inhibitors and progression of nondiabetic renal disease: A meta-analysis of patient-level data. Ann Intern Med 135: 73–87, 2001 - PubMed
-
- Hocher B, Schwarz A, Reinbacher D, Jacobi J, Lun A, Priem F: Effects of endothelin receptor antagonists on the progression of diabetic nephropathy. Nephron 87: 161–169, 2001 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
