

Tumor invasion after treatment of glioblastoma with bevacizumab: radiographic and pathologic correlation in humans and mice
- PMID: 20167811
- PMCID: PMC2940588
- DOI: 10.1093/neuonc/nop027
Tumor invasion after treatment of glioblastoma with bevacizumab: radiographic and pathologic correlation in humans and mice
Abstract
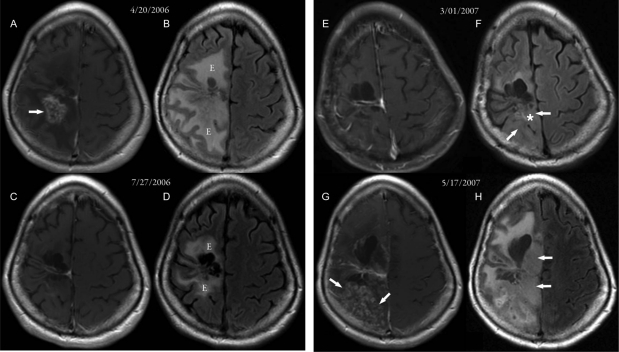
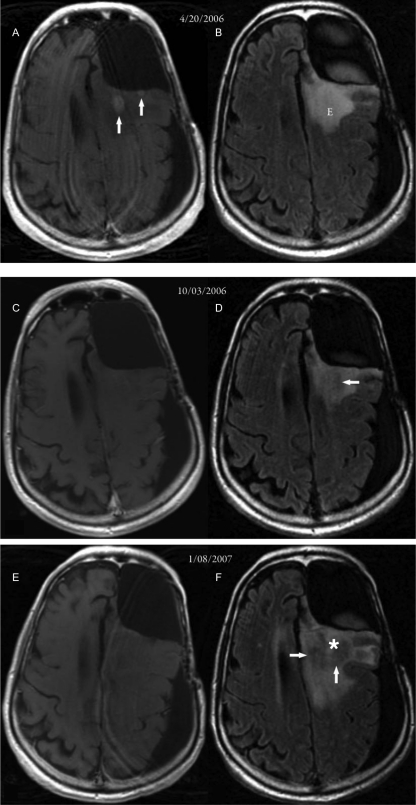
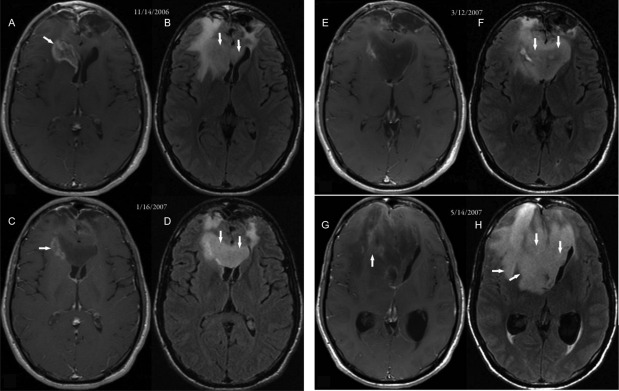
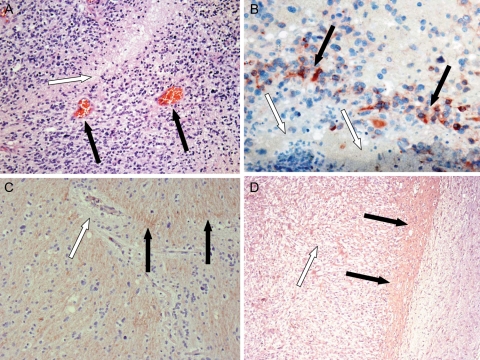
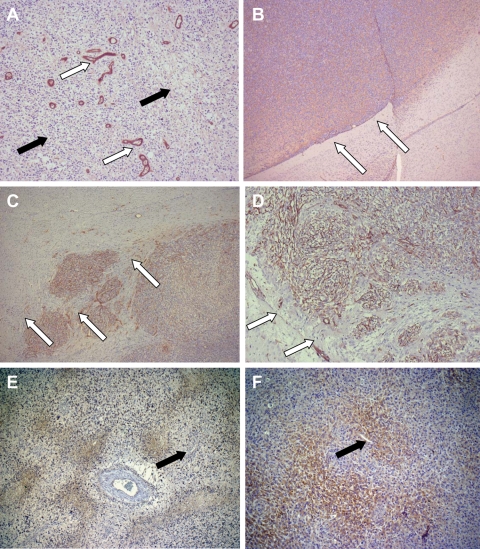
Patients with recurrent malignant glioma treated with bevacizumab, a monoclonal antibody to vascular endothelial growth factor (VEGF), alone or in combination with irinotecan have had impressive reductions in MRI contrast enhancement and vasogenic edema. Responses to this regimen, as defined by a decrease in contrast enhancement, have led to significant improvements in progression-free survival rates but not in overall survival duration. Some patients for whom this treatment regimen fails have an uncharacteristic pattern of tumor progression, which can be observed radiographically as an increase in hyperintensity on T2-weighted or fluid-attenuated inverse recovery (FLAIR) MRI. To date, there have been no reports of paired correlations between radiographic results and histopathologic findings describing the features of this aggressive tumor phenotype. In this study, we correlate such findings for 3 illustrative cases of gliomas that demonstrated an apparent phenotypic shift to a predominantly infiltrative pattern of tumor progression after treatment with bevacizumab. Pathologic examination of abnormal FLAIR areas on MRI revealed infiltrative tumor with areas of thin-walled blood vessels, suggesting vascular "normalization," which was uncharacteristically adjacent to regions of necrosis. High levels of insulin-like growth factor binding protein-2 and matrix metalloprotease-2 expression were seen within the infiltrating tumor. In an attempt to better understand this infiltrative phenotype associated with anti-VEGF therapy, we forced a highly angiogenic, noninvasive orthotopic U87 xenograft tumor to become infiltrative by treating the mice with bevacizumab. This model mimicked many of the histopathologic findings from the human cases and will augment the discovery of alternative or additive therapies to prevent this type of tumor recurrence in clinical practice.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–996. - PubMed
-
- Wong ET, Hess KR, Gleason MJ, et al. Outcomes and prognostic factors in recurrent glioma patients enrolled onto phase II clinical trials. J Clin Oncol. 1999;17:2572–2578. - PubMed
-
- Curran WJ, Jr, Scott CB, Horton J, et al. Recursive partitioning analysis of prognostic factors in three Radiation Therapy Oncology Group malignant glioma trials. J Natl Cancer Inst. 1993;85:704–710. - PubMed
-
- Millauer B, Shawver LK, Plate KH, Risau W, Ullrich A. Glioblastoma growth inhibited in vivo by a dominant-negative Flk-1 mutant. Nature. 1994;367:576–579. - PubMed
-
- Folkman J. Tumor angiogenesis. Adv Cancer Res. 1985;43:175–203. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
