

High-dose carboplatin, thiotepa, and etoposide with autologous stem cell rescue for patients with previously irradiated recurrent medulloblastoma
- PMID: 20167818
- PMCID: PMC2940591
- DOI: 10.1093/neuonc/nop031
High-dose carboplatin, thiotepa, and etoposide with autologous stem cell rescue for patients with previously irradiated recurrent medulloblastoma
Abstract
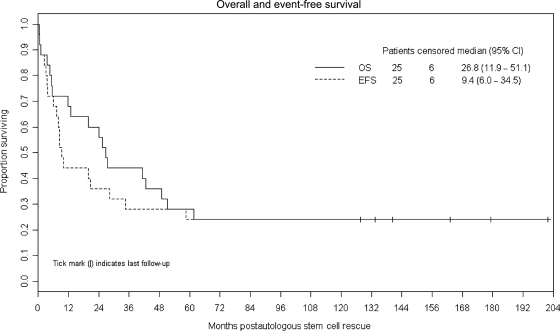
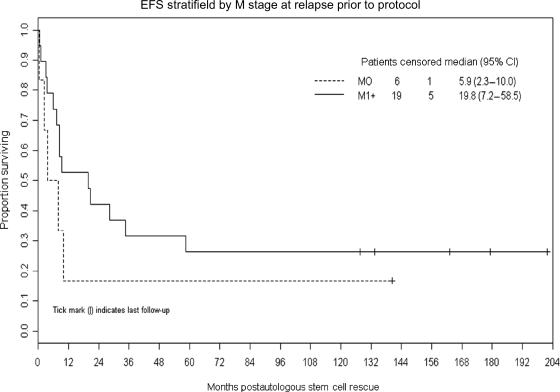
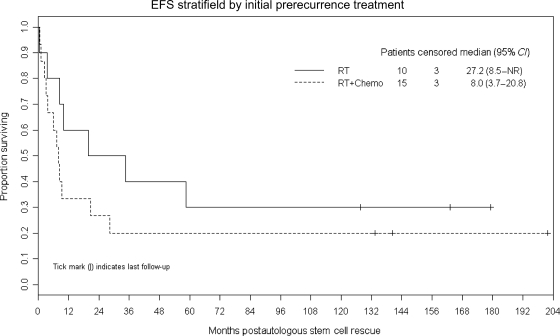
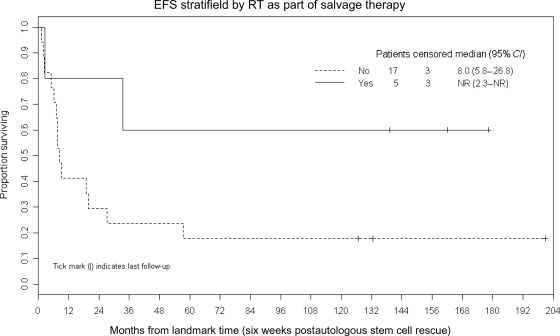
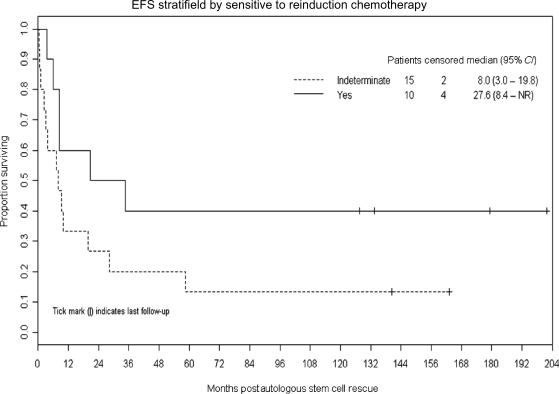
Recurrent medulloblastoma is highly lethal in previously irradiated patients. Previously irradiated patients with M-0-M-3 recurrences who achieved a minimal disease state prior to protocol enrollment received carboplatin (Calvert formula with area under the curve = 7 mg/mL min, maximum 500 mg/m(2)/day) on days -8 to -6, and thiotepa (300 mg/m(2)/day) and etoposide (250 mg/m(2)/day) on days -5 to -3, followed by autologous stem cell rescue (ASCR) on day 0. Twenty-five patients, aged 7.6-44.7 years (median 13.8 years) at ASCR, were treated. Three (12%) died of treatment-related toxicities within 30 days of ASCR, due to multiorgan system failure (n = 2) and aspergillus infection with veno-occlusive disease (n = 1). Tumor recurred in 16 at a median of 8.5 months (range 2.3-58.5 months). Six are event-free survivors at a median of 151.2 months post-ASCR (range 127.2-201.6 months). The Kaplan-Meier estimate of median overall survival is 26.8 months (95% CI: 11.9-51.1 months) and of event-free survival (EFS) and overall survival are both 24% (95% CI: 9.8%-41.7%) at 10 years post-ASCR. M-0 (vs M-1 + ) recurrence prior to protocol, lack of tissue confirmation of relapse, and initial therapy of radiation therapy (RT) alone (vs RT + chemotherapy) were not significantly associated with better EFS (P = .33, .34, and .27, respectively). Trends toward better EFS were noted in patients (n = 5) who received additional RT as part of their retrieval therapy (P = .07) and whose recurrent disease was demonstrated to be sensitive to reinduction chemotherapy (P = .09). This retrieval strategy provides long-term EFS for some patients with previously irradiated recurrent medulloblastoma. The use of additional RT may be associated with better outcome.
Figures
References
-
- Packer RJ, Gajjar A, Vezina G, et al. Phase III study of craniospinal radiation therapy followed by adjuvant chemotherapy for newly diagnosed average-risk medulloblastoma. J Clin Oncol. 2006;24:4202–4208. - PubMed
-
- Gajjar A, Chintagumpala M, Ashley D, et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): long-term results from a prospective, multicentre trial. Lancet Oncol. 2006;7:813–820. - PubMed
-
- Belza MG, Donaldson SS, Steinberg GK, Cox RS, Cogen PH. Medulloblastoma: freedom from relapse longer than 8 years—a therapeutic cure? J Neurosurg. 1991;75:575–582. - PubMed
-
- Torres CF, Rebsamen S, Silber JH, et al. Surveillance scanning of children with medulloblastoma. N Engl J Med. 1994;330:892–895. - PubMed
-
- Dunkel IJ, Boyett JM, Yates A, et al. High dose carboplatin, thiotepa and etoposide with autologous stem cell rescue for patients with recurrent medulloblastoma. J Clin Oncol. 1998;16:222–228. - PubMed
