

Assessment and optimization of cell engraftment after transplantation into the heart
- PMID: 20167944
- PMCID: PMC2826722
- DOI: 10.1161/CIRCRESAHA.109.208991
Assessment and optimization of cell engraftment after transplantation into the heart
Abstract
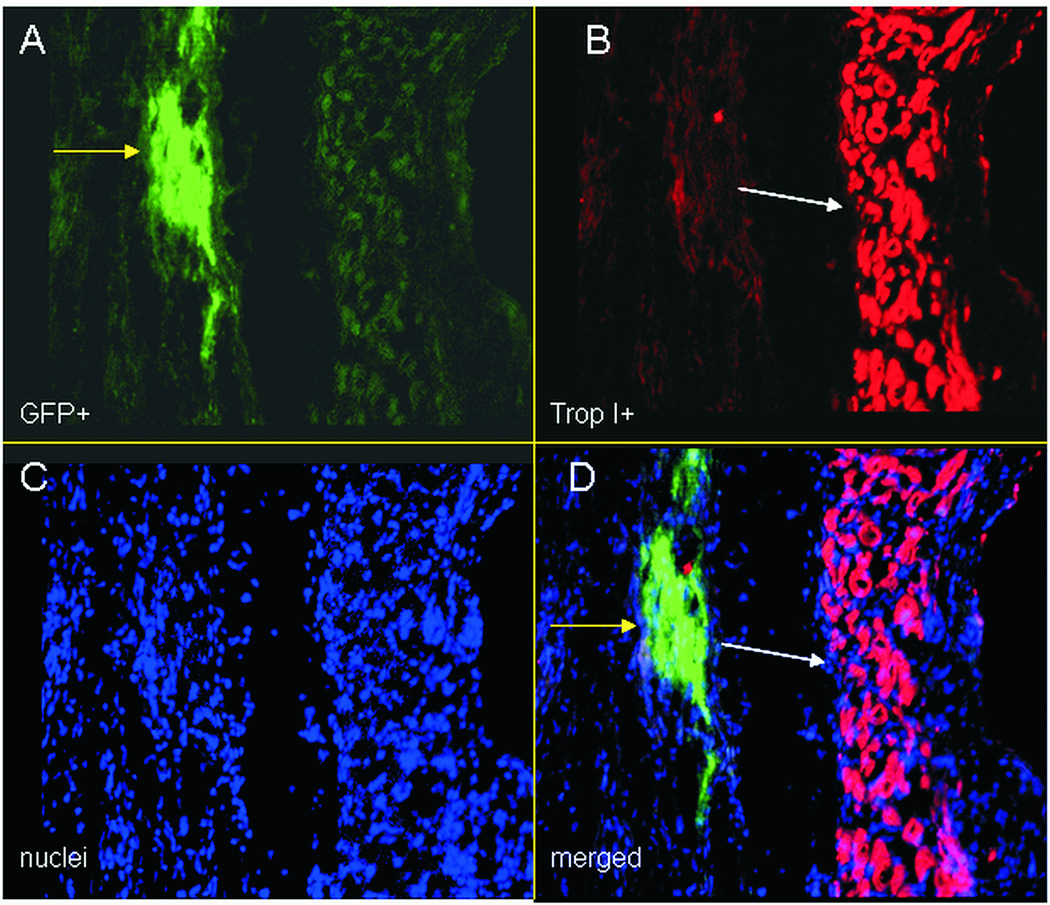
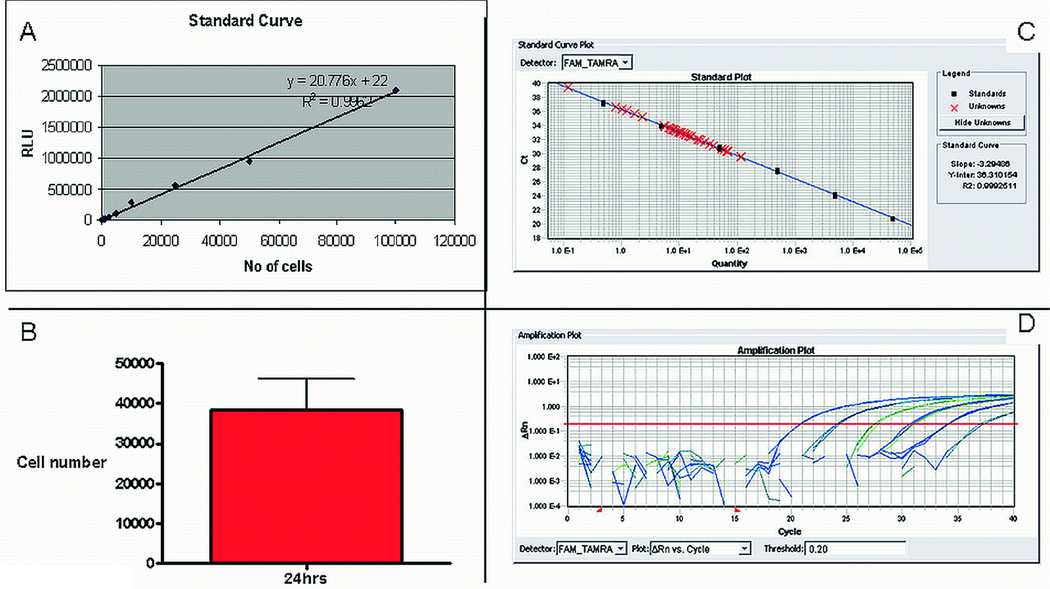
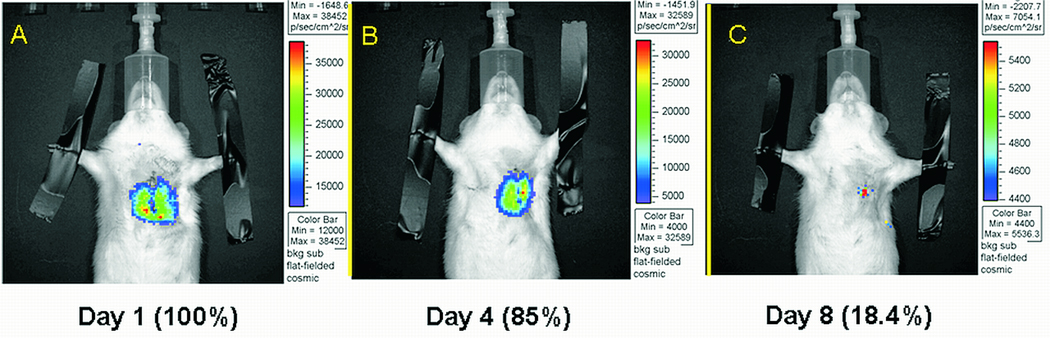
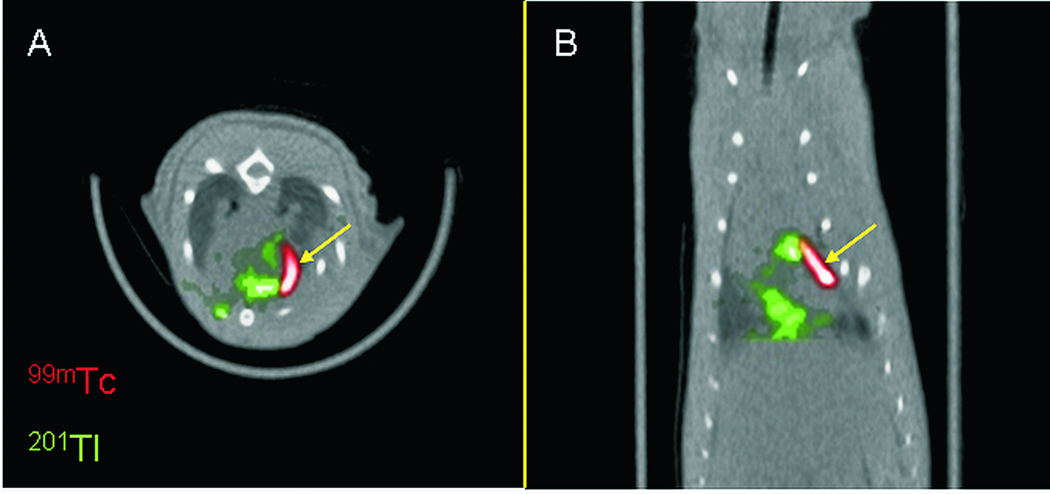
Myocardial regeneration using stem and progenitor cell transplantation in the injured heart has recently become a major goal in the treatment of cardiac disease. Experimental studies and clinical applications have generally been encouraging, although the functional benefits that have been attained clinically are modest and inconsistent. Low cell retention and engraftment after myocardial delivery is a key factor limiting the successful application of cell therapy, irrespective of the type of cell or the delivery method. To improve engraftment, accurate methods for tracking cell fate and quantifying cell survival need to be applied. Several laboratory techniques (histological methods, real-time quantitative polymerase chain reaction, radiolabeling) have provided invaluable information about cell engraftment. In vivo imaging (nuclear medicine modalities, bioluminescence, and MRI) has the potential to provide quantitative information noninvasively, enabling longitudinal assessment of cell fate. In the present review, we present several available methods for assessing cell engraftment, and we critically discuss their strengths and limitations. In addition to providing insights about the mechanisms mediating cell loss after transplantation, these methods can evaluate techniques for augmenting engraftment, such as tissue engineering approaches, preconditioning, and genetic modification, allowing optimization of cell therapies.
Figures




Similar articles
-
Transplantation and tracking of human-induced pluripotent stem cells in a pig model of myocardial infarction: assessment of cell survival, engraftment, and distribution by hybrid single photon emission computed tomography/computed tomography of sodium iodide symporter transgene expression.Circulation. 2012 Jul 24;126(4):430-9. doi: 10.1161/CIRCULATIONAHA.111.087684. Epub 2012 Jul 5. Circulation. 2012. PMID: 22767659
-
Early stem cell engraftment predicts late cardiac functional recovery: preclinical insights from molecular imaging.Circ Cardiovasc Imaging. 2012 Jul;5(4):481-90. doi: 10.1161/CIRCIMAGING.111.969329. Epub 2012 May 7. Circ Cardiovasc Imaging. 2012. PMID: 22565608 Free PMC article.
-
Direct evaluation of myocardial viability and stem cell engraftment demonstrates salvage of the injured myocardium.Circ Res. 2015 Mar 27;116(7):e40-50. doi: 10.1161/CIRCRESAHA.116.304668. Epub 2015 Feb 5. Circ Res. 2015. PMID: 25654979 Free PMC article.
-
Cell delivery and tracking in post-myocardial infarction cardiac stem cell therapy: an introduction for clinical researchers.Heart Fail Rev. 2010 Jan;15(1):1-14. doi: 10.1007/s10741-009-9134-1. Heart Fail Rev. 2010. PMID: 19238541 Review.
-
Molecular imaging in stem cell-based therapies of cardiac diseases.Adv Drug Deliv Rev. 2017 Oct 1;120:71-88. doi: 10.1016/j.addr.2017.07.012. Epub 2017 Jul 19. Adv Drug Deliv Rev. 2017. PMID: 28734900 Review.
Cited by
-
All Roads Lead to Rome (the Heart): Cell Retention and Outcomes From Various Delivery Routes of Cell Therapy Products to the Heart.J Am Heart Assoc. 2021 Apr 20;10(8):e020402. doi: 10.1161/JAHA.120.020402. Epub 2021 Apr 6. J Am Heart Assoc. 2021. PMID: 33821664 Free PMC article. Review.
-
Programming and reprogramming a human heart cell.EMBO J. 2015 Mar 12;34(6):710-38. doi: 10.15252/embj.201490563. Epub 2015 Feb 20. EMBO J. 2015. PMID: 25712211 Free PMC article. Review.
-
Injectable Hydrogels with In Situ Double Network Formation Enhance Retention of Transplanted Stem Cells.Adv Funct Mater. 2015 Mar 4;25(9):1344-1351. doi: 10.1002/adfm.201403631. Adv Funct Mater. 2015. PMID: 26273242 Free PMC article. No abstract available.
-
Icariin induces mouse embryonic stem cell differentiation into beating functional cardiomyocytes.Mol Cell Biochem. 2011 Mar;349(1-2):117-23. doi: 10.1007/s11010-010-0666-4. Epub 2010 Dec 23. Mol Cell Biochem. 2011. PMID: 21181238
-
Nanovector-based prolyl hydroxylase domain 2 silencing system enhances the efficiency of stem cell transplantation for infarcted myocardium repair.Int J Nanomedicine. 2014 Nov 11;9:5203-15. doi: 10.2147/IJN.S71586. eCollection 2014. Int J Nanomedicine. 2014. PMID: 25429216 Free PMC article.
References
-
- Segers VF, Lee RT. Stem-cell therapy for cardiac disease. Nature. 2008;451:937–942. - PubMed
-
- Abdel-Latif A, Bolli R, Tleyjeh IM, Montori VM, Perin EC, Hornung CA, Zuba-Surma EK, Al-Mallah M, Dawn B. Adult bone marrow-derived cells for cardiac repair: a systematic review and meta-analysis. Arch Intern Med. 2007;167:989–997. - PubMed
-
- Mazhari R, Hare JM. Advances in cell-based therapy for structural heart disease. Prog Cardiovasc Dis. 2007;49:387–395. - PubMed
-
- Lipinski MJ, Biondi-Zoccai GG, Abbate A, Khianey R, Sheiban I, Bartunek J, Vanderheyden M, Kim HS, Kang HJ, Strauer BE, Vetrovec GW. Impact of intracoronary cell therapy on left ventricular function in the setting of acute myocardial infarction: a collaborative systematic review and meta-analysis of controlled clinical trials. J Am Coll Cardiol. 2007;50:1761–1767. - PubMed
-
- Wollert KC, Drexler H. Clinical applications of stem cells for the heart. Circ.Res. 2005;96:151–163. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
