

Accuracy of retinopathy of prematurity diagnosis by retinal fellows
- PMID: 20168274
- PMCID: PMC2884082
- DOI: 10.1097/IAE.0b013e3181c9696a
Accuracy of retinopathy of prematurity diagnosis by retinal fellows
Abstract
Purpose: The purpose of this study was to measure the accuracy of retinopathy of prematurity (ROP) diagnosis by retinal fellows.
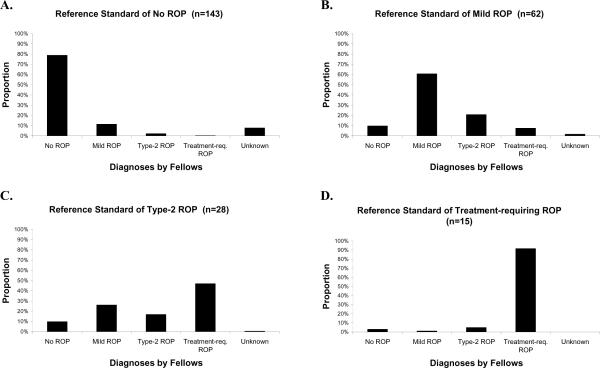
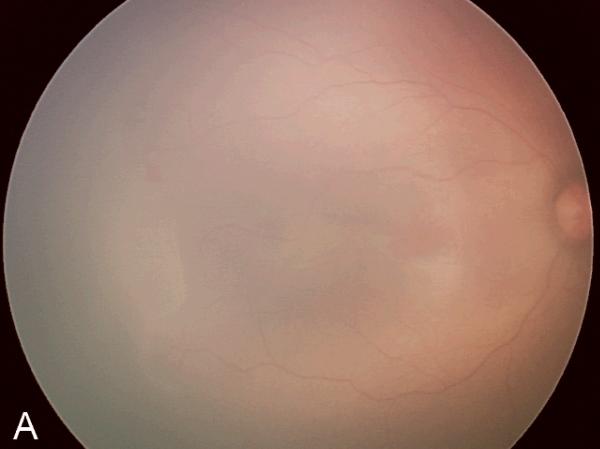
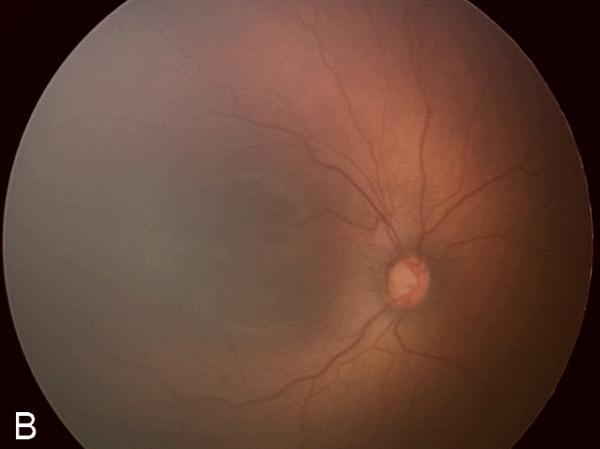
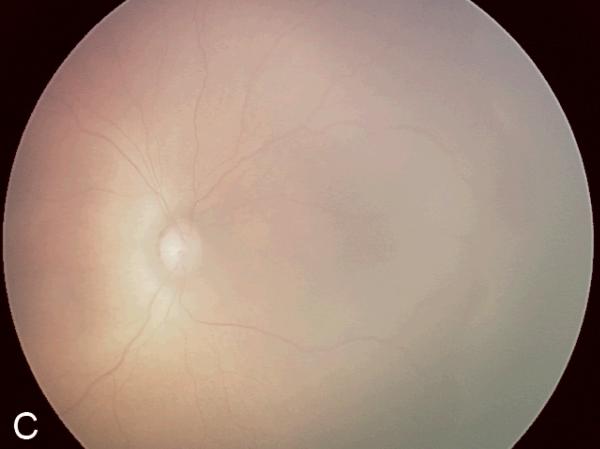
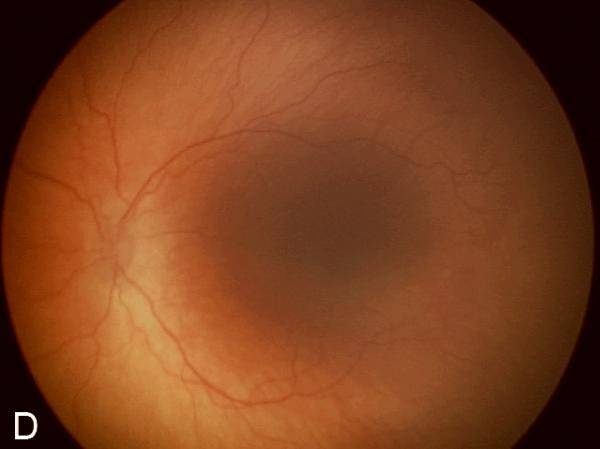
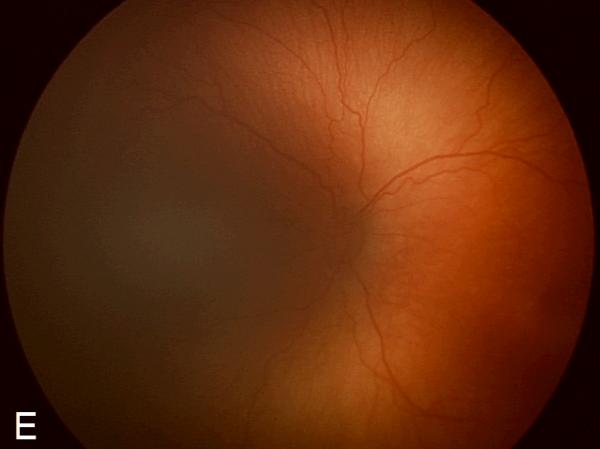
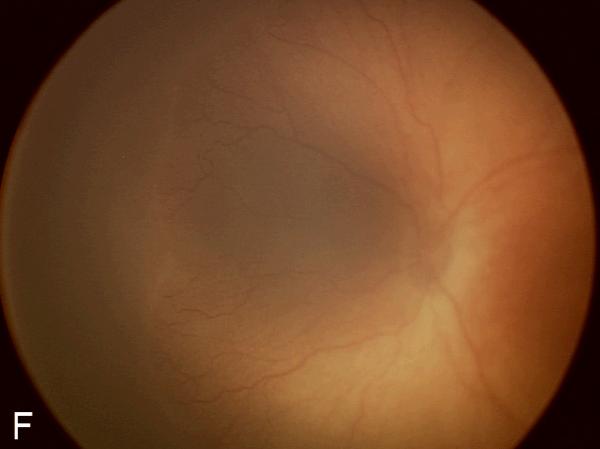
Methods: An atlas of 804 retinal images was captured from 248 eyes of 67 premature infants with a wide-angle camera (RetCam-II, Clarity Medical Systems, Pleasanton, CA). Images were uploaded to a study Web site, from which an expert pediatric retinal specialist and 7 retinal fellows independently provided a diagnosis (no ROP, mild ROP, type 2 ROP, or treatment-requiring ROP) for each eye. The sensitivity and specificity of each retinal fellow were calculated and subsequently compared with a reference standard of diagnosis by an expert pediatric retinal specialist.
Results: For detection of type 2 or worse ROP by fellows, mean (range) sensitivity was 0.751 (0.512-0.953), and specificity was 0.841 (0.707-0.976). For detection of treatment-requiring ROP, mean (range) sensitivity was 0.914 (0.667-1.000), and specificity was 0.871 (0.678-0.987).
Conclusion: In general, fellows showed high accuracy for detecting ROP. However, 3 of 7 fellows achieved <80% sensitivity for diagnosis of type 2 or worse ROP, and 2 of 7 achieved <90% sensitivity for diagnosis of treatment-requiring ROP. This could lead to undermanagement and undertreatment of clinically significant disease and raises potential concerns about the quality of ROP screening examinations performed by less-experienced examiners.
Figures
References
-
- Flynn JT, Bancalari E, Bachynski BN, et al. Retinopathy of prematurity. Diagnosis, severity, and natural history. Ophthalmology. 1987;94:620–629. - PubMed
-
- Martin JA, Hamilton BE, Sutton PD, et al. Births: final data for 2005. Natl Vital Stat Rep. 2007;56:1–103. - PubMed
-
- National Eye Institute Retinopathy of Prematurity. [Accessed May 16, 2008]. Available at: http://www.nei.nih.gov/health/rop/.
-
- Phelps DL. Retinopathy of prematurity: an estimate of vision loss in the United State—1979. Pediatrics. 1981;67:924–925. - PubMed
-
- Multicenter trial of cryotherapy for retinopathy of prematurity. Preliminary results. Cryotherapy for Retinopathy of Prematurity Cooperative Group. Arch Ophthalmol. 1988;106:471–479. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
