

Accuracy of different methods for blood glucose measurement in critically ill patients
- PMID: 20169273
- PMCID: PMC11553116
- DOI: 10.1590/s1516-31802009000500003
Accuracy of different methods for blood glucose measurement in critically ill patients
Abstract
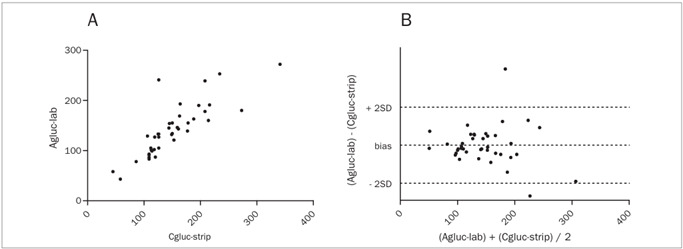
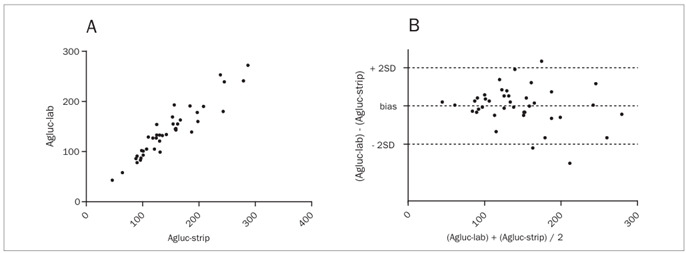
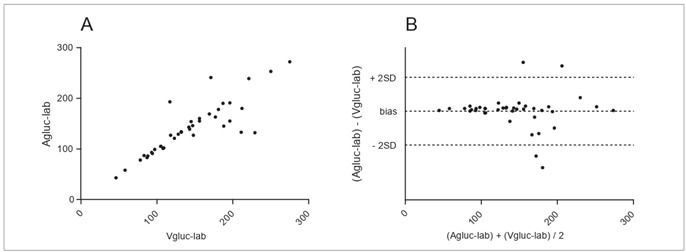
Context and objective: Although glucometers have not been validated for intensive care units, they are regularly used. The aim of this study was to compare and assess the accuracy and clinical agreement of arterial glucose concentration obtained using colorimetry (Agluc-lab), capillary (Cgluc-strip) and arterial (Agluc-strip) glucose concentration obtained using glucometry and central venous glucose concentration obtained using colorimetry (Vgluc-lab).
Design and setting: Cross-sectional study in a university hospital.
Method: Forty patients with septic shock and stable individuals without infection were included. The correlations between measurements were assessed both in the full sample and in subgroups using noradrenalin and presenting signs of tissue hypoperfusion.
Results: Cgluc-strip showed the poorest correlation (r = 0.8289) and agreement (-9.87 +/- 31.76). It exceeded the limits of acceptable variation of the Clinical and Laboratory Standards Institute in 23.7% of the cases, and was higher than Agluc-lab in 90% of the measurements. Agluc-strip showed the best correlation (r = 0.9406), with agreement of -6.75 +/- 19.07 and significant variation in 7.9%. For Vgluc-lab, r = 0.8549, with agreement of -4.20 +/- 28.37 and significant variation in 15.7%. Significant variation was more frequent in patients on noradrenalin (36.4% versus 6.3%; P = 0.03) but not in the subgroup with hypoperfusion. There was discordance regarding clinical management in 25%, 22% and 15% of the cases for Cgluc-strip, Vgluc-lab and Agluc-strip, respectively.
Conclusion: Cgluc-strip should be avoided, particularly if noradrenalin is being used. This method usually overestimates the true glucose levels and gives rise to management errors.
Clinical trial registration: ACTRN12608000513314 (registered as an observational, cross-sectional study).
CONTEXTO E OBJETIVO:: Apesar de glicosímetros não serem validados para unidades de terapia intensiva (UTI), seu uso é corriqueiro. O objetivo foi avaliar a acurácia e concordância clínica entre a glicemia arterial por colorimetria (glicA-lab), glicemias capilar (glicC-fita) e arterial (glicA-fita) por glicosimetria, e venosa central por colorimetria (glicV-lab).
TIPO DE ESTUDO E LOCAL:: Estudo transversal realizado em hospital universitário.
MÉTODO:: Foram incluídos 40 pacientes com choque séptico e indivíduos estáveis, sem infecção. A correlação entre medidas foi avaliada tanto na amostra global quanto nos subgrupos em uso de noradrenalina e com sinais de hipoperfusão tecidual.
RESULTADOS:: A glicC-fita mostrou pior correlação (r = 0,8289) e concordância (-9,87 ± 31,76). Esta superou os limites aceitáveis de variação do Clinical and Laboratory Standards Institute em 23,7% dos casos, sendo maior que a glicA-lab em 90% das vezes. A glicA-fita teve a melhor correlação (r = 0,9406), com concordância de -6,75 ± 19,07 e variação significativa em 7,9%. Para a glicV-lab, obteve-se r = 0,8549, concordância de -4,20 ± 28,37 e variação significativa em 15,7%. Variação significativa foi mais frequente em pacientes com noradrenalina (36,4% versus 6,3%, P = 0,03), mas não nos com hipoperfusão. Houve discordância de conduta clínica em 25%, 22,5% e 15% dos casos para glicC-fita, glicV-lab e glicA-fita, respectivamente.
CONCLUSÃO:: O uso de glicC-fita deveria ser evitado, principalmente se há uso de noradrenalina. Geralmente, este método superestima a glicemia real e acarreta erros de conduta.
REGISTRO DO ENSAIO CLÍNICO:: ACTRN12608000513314 (registrado como estudo observacional transversal)
Conflict of interest statement
Figures
Similar articles
-
Accuracy of bedside glucometry in critically ill children with peripheral hypoperfusion.J Clin Monit Comput. 2015 Feb;29(1):145-52. doi: 10.1007/s10877-014-9579-1. Epub 2014 May 7. J Clin Monit Comput. 2015. PMID: 24801361
-
Fingerstick glucose determination in shock.Ann Intern Med. 1991 Jun 15;114(12):1020-4. doi: 10.7326/0003-4819-114-12-1020. Ann Intern Med. 1991. PMID: 2029097
-
Bedside blood glucose determinations in critical care medicine: a comparative analysis of two techniques.Crit Care Med. 1982 Jul;10(7):463-5. doi: 10.1097/00003246-198207000-00012. Crit Care Med. 1982. PMID: 7083872
-
Inaccuracy of Venous Point-of-Care Glucose Measurements in Critically Ill Patients: A Cross-Sectional Study.PLoS One. 2015 Jun 12;10(6):e0129568. doi: 10.1371/journal.pone.0129568. eCollection 2015. PLoS One. 2015. PMID: 26067093 Free PMC article.
-
Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012.Crit Care Med. 2013 Feb;41(2):580-637. doi: 10.1097/CCM.0b013e31827e83af. Crit Care Med. 2013. PMID: 23353941
Cited by
-
Accuracy of blood glucose measurements using the NOVA StatStrip® glucometer during cardiac surgery: a prospective observational study.Can J Anaesth. 2019 Aug;66(8):943-952. doi: 10.1007/s12630-019-01350-7. Epub 2019 Mar 20. Can J Anaesth. 2019. PMID: 30895515 Clinical Trial. English.
-
Association between Blood Glucose and cardiac Rhythms during pre-hospital care of Trauma Patients - a retrospective Analysis.Scand J Trauma Resusc Emerg Med. 2018 Jul 13;26(1):58. doi: 10.1186/s13049-018-0516-z. Scand J Trauma Resusc Emerg Med. 2018. PMID: 30005711 Free PMC article.
-
Effect of D-glucose feeding on mortality induced by sepsis.Korean J Physiol Pharmacol. 2016 Jan;20(1):83-9. doi: 10.4196/kjpp.2016.20.1.83. Epub 2015 Dec 31. Korean J Physiol Pharmacol. 2016. PMID: 26807027 Free PMC article.
-
Accuracy and Precision of Measured Blood Sugar Values by Three Glucometers Compared to the Standard Technique.J Clin Diagn Res. 2017 Apr;11(4):OC05-OC08. doi: 10.7860/JCDR/2017/23926.9613. Epub 2017 Apr 1. J Clin Diagn Res. 2017. PMID: 28571181 Free PMC article.
-
Hypoglycemia in critically ill children.J Diabetes Sci Technol. 2012 Jan 1;6(1):48-57. doi: 10.1177/193229681200600107. J Diabetes Sci Technol. 2012. PMID: 22401322 Free PMC article.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303–1310. - PubMed
-
- Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004;32(3):858–873. - PubMed
-
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368–1377. - PubMed
-
- Vanhorebeek I, Langouche L, Van den Berghe G. Tight blood glucose control with insulin in the ICU: facts and controversies. Chest. 2007;132(1):268–278. - PubMed
-
- Mebis L, Gunst J, Langouche L, Vanhorebeek I, Van den Berghe G. Indication and practical use of intensive insulin therapy in the critically ill. Curr Opin Crit Care. 2007;13(4):392–398. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
