

Different screening strategies (single or dual) for the diagnosis of suspected latent tuberculosis: a cost effectiveness analysis
- PMID: 20170555
- PMCID: PMC2837635
- DOI: 10.1186/1471-2466-10-7
Different screening strategies (single or dual) for the diagnosis of suspected latent tuberculosis: a cost effectiveness analysis
Abstract
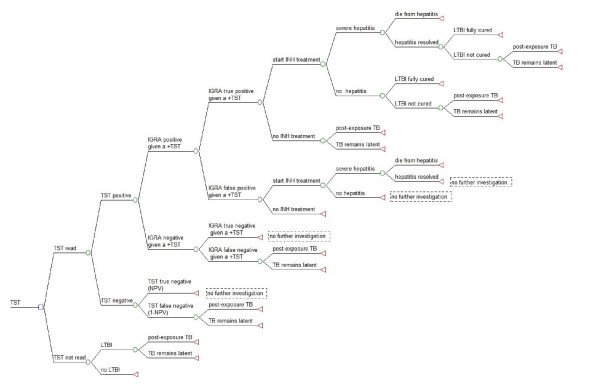
Background: Previous health economic studies recommend either a dual screening strategy [tuberculin skin test (TST) followed by interferon-gamma-release assay (IGRA)] or a single one [IGRA only] for latent tuberculosis infection (LTBI), the former largely based on claims that it is more cost-effective. We sought to examine that conclusion through the use of a model that accounts for the additional costs of adverse drug reactions and directly compares two commercially available versions of the IGRA: the Quantiferon-TB-Gold-In-Tube (QFT-GIT) and T-SPOT.TB.
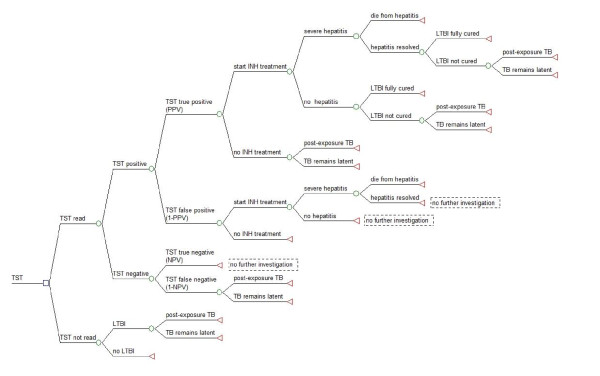
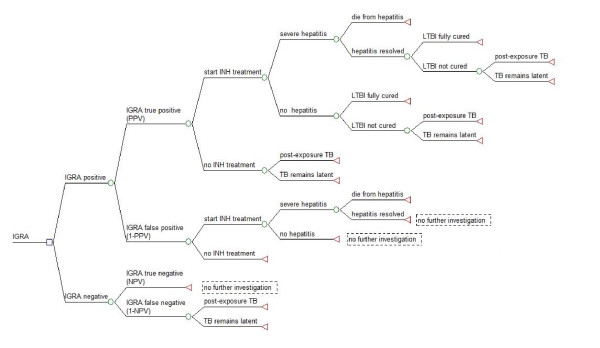
Methods: A LTBI screening model directed at screening contacts was used to perform a cost-effectiveness analysis, from a UK healthcare perspective, taking into account the risk of isoniazid-related hepatotoxicity and post-exposure TB (2 years post contact) using the TST, QFT-GIT and T-SPOT.TB IGRAs.
Results: Examining costs alone, the TST/IGRA dual screening strategies (TST/T-SPOT.TB and TST/QFT-GIT; 162,387 pounds and 157,048 pounds per 1000 contacts, respectively) cost less than their single strategy counterparts (T-SPOT.TB and QFT-GIT; 203,983 pounds and 202,921 pounds per 1000 contacts) which have higher IGRA test costs and greater numbers of persons undergoing LTBI treatment. However, IGRA alone strategies direct healthcare interventions and costs more accurately to those that are truly infected.Subsequently, less contacts need to be treated to prevent an active case of TB (T-SPOT.TB and QFT-GIT; 61.7 and 69.7 contacts) in IGRA alone strategies. IGRA single strategies also prevent more cases of post-exposure TB. However, this greater effectiveness does not outweigh the lower incremental costs associated with the dual strategies. Consequently, when these costs are combined with effectiveness, the IGRA dual strategies are more cost-effective than their single strategy counterparts. Comparing between the IGRAs, T-SPOT.TB-based strategies (single and dual; 39,712 pounds and 37,206 pounds per active TB case prevented, respectively) were more cost-effective than the QFT-GIT-based strategies (single and dual; 42,051 pounds and 37,699 pounds per active TB case prevented, respectively). Using the TST alone was the least cost-effective (47,840 pounds per active TB case prevented). Cost effectiveness values were sensitive to changes in LTBI prevalence, IGRA test sensitivities/specificities and IGRA test costs.
Conclusion: A dual strategy is more cost effective than a single strategy but this conclusion is sensitive to screening test assumptions and LTBI prevalence.
Figures
Similar articles
-
Cost-effectiveness of Quantiferon®-TB Gold-in-Tube versus tuberculin skin testing for contact screening and treatment of latent tuberculosis infection in Brazil.PLoS One. 2013 Apr 4;8(4):e59546. doi: 10.1371/journal.pone.0059546. Print 2013. PLoS One. 2013. PMID: 23593145 Free PMC article.
-
Two interferon gamma release assays for predicting active tuberculosis: the UK PREDICT TB prognostic test study.Health Technol Assess. 2018 Oct;22(56):1-96. doi: 10.3310/hta22560. Health Technol Assess. 2018. PMID: 30334521 Free PMC article.
-
Systematic review of cost and cost-effectiveness of different TB-screening strategies.BMC Health Serv Res. 2011 Sep 30;11:247. doi: 10.1186/1472-6963-11-247. BMC Health Serv Res. 2011. PMID: 21961888 Free PMC article.
-
Interferon gamma release assays for Diagnostic Evaluation of Active tuberculosis (IDEA): test accuracy study and economic evaluation.Health Technol Assess. 2019 May;23(23):1-152. doi: 10.3310/hta23230. Health Technol Assess. 2019. PMID: 31138395 Free PMC article.
-
Interferon-Gamma Release Assay Testing for Latent Tuberculosis Infection: A Health Technology Assessment.Ont Health Technol Assess Ser. 2024 Dec 12;24(11):1-183. eCollection 2024. Ont Health Technol Assess Ser. 2024. PMID: 39911267 Free PMC article.
Cited by
-
Predictive value of the tuberculin skin test among newly arriving immigrants.PLoS One. 2013;8(3):e60130. doi: 10.1371/journal.pone.0060130. Epub 2013 Mar 27. PLoS One. 2013. PMID: 23544128 Free PMC article.
-
Relevance and acceptability of using the Quantiferon gold test (QGIT) to screen CD4 blood draws for latent TB infection among PLHIV in South Africa: formative qualitative research findings from the TEKO trial.BMC Health Serv Res. 2018 Apr 16;18(1):288. doi: 10.1186/s12913-018-3088-8. BMC Health Serv Res. 2018. PMID: 29661197 Free PMC article.
-
Cost-effectiveness of Quantiferon®-TB Gold-in-Tube versus tuberculin skin testing for contact screening and treatment of latent tuberculosis infection in Brazil.PLoS One. 2013 Apr 4;8(4):e59546. doi: 10.1371/journal.pone.0059546. Print 2013. PLoS One. 2013. PMID: 23593145 Free PMC article.
-
Management of latent Mycobacterium tuberculosis infection: WHO guidelines for low tuberculosis burden countries.Eur Respir J. 2015 Dec;46(6):1563-76. doi: 10.1183/13993003.01245-2015. Epub 2015 Sep 24. Eur Respir J. 2015. PMID: 26405286 Free PMC article. Review.
-
Cost-effectiveness analysis of community active case finding and household contact investigation for tuberculosis case detection in urban Africa.PLoS One. 2015 Feb 6;10(2):e0117009. doi: 10.1371/journal.pone.0117009. eCollection 2015. PLoS One. 2015. PMID: 25658592 Free PMC article.
References
-
- Menzies D, Pai M, Comstock G. Meta-analysis: new tests for the diagnosis of latent tuberculosis infection: areas of uncertainty and recommendations for research. Annals of internal medicine. 2007;146(5):340–354. - PubMed
-
- Farhat M, Greenaway C, Pai M, Menzies D. False-positive tuberculin skin tests: what is the absolute effect of BCG and non-tuberculous mycobacteria? Int J Tuberc Lung Dis. 2006;10(11):1192–1204. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
