

The absence of coronary calcification does not exclude obstructive coronary artery disease or the need for revascularization in patients referred for conventional coronary angiography
- PMID: 20170786
- PMCID: PMC3294287
- DOI: 10.1016/j.jacc.2009.07.072
The absence of coronary calcification does not exclude obstructive coronary artery disease or the need for revascularization in patients referred for conventional coronary angiography
Abstract
Objectives: This study was designed to evaluate whether the absence of coronary calcium could rule out >or=50% coronary stenosis or the need for revascularization.
Background: The latest American Heart Association guidelines suggest that a calcium score (CS) of zero might exclude the need for coronary angiography among symptomatic patients.
Methods: A substudy was made of the CORE64 (Coronary Evaluation Using Multi-Detector Spiral Computed Tomography Angiography Using 64 Detectors) multicenter trial comparing the diagnostic performance of 64-detector computed tomography to conventional angiography. Patients clinically referred for conventional angiography were asked to undergo a CS scan up to 30 days before.
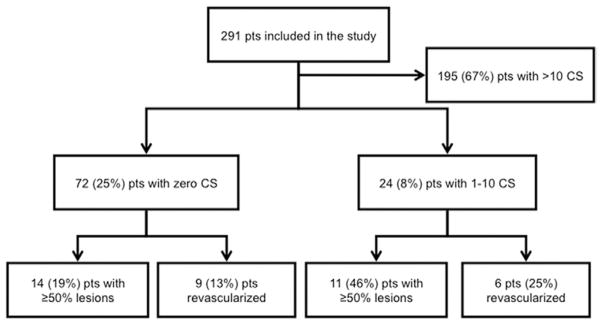
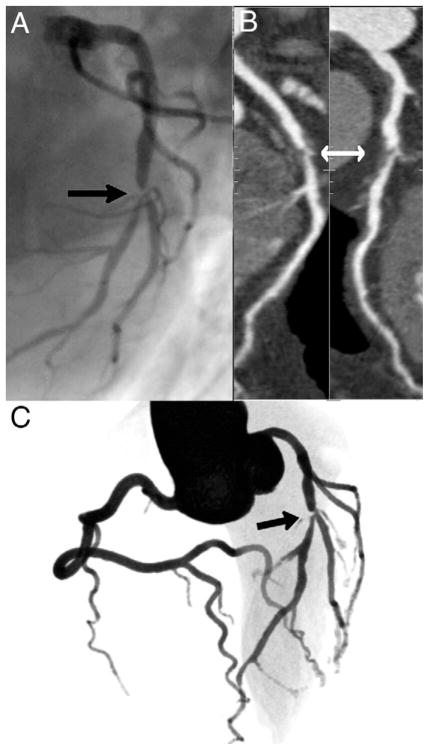
Results: In all, 291 patients were included, of whom 214 (73%) were male, and the mean age was 59.3 +/- 10.0 years. A total of 14 (5%) patients had low, 218 (75%) had intermediate, and 59 (20%) had high pre-test probability of obstructive coronary artery disease. The overall prevalence of >or=50% stenosis was 56%. A total of 72 patients had CS = 0, among whom 14 (19%) had at least 1 >or=50% stenosis. The overall sensitivity for CS = 0 to predict the absence of >or=50% stenosis was 45%, specificity was 91%, negative predictive value was 68%, and positive predictive value was 81%. Additionally, revascularization was performed in 9 (12.5%) CS = 0 patients within 30 days of the CS. From a total of 383 vessels without any coronary calcification, 47 (12%) presented with >or=50% stenosis; and from a total of 64 totally occluded vessels, 13 (20%) had no calcium.
Conclusions: The absence of coronary calcification does not exclude obstructive stenosis or the need for revascularization among patients with high enough suspicion of coronary artery disease to be referred for coronary angiography, in contrast with the published recommendations. Total coronary occlusion frequently occurs in the absence of any detectable calcification. (Coronary Evaluation Using Multi-Detector Spiral Computed Tomography Angiography Using 64 Detectors [CORE-64]; NCT00738218).
Figures
Comment in
-
Zero coronary calcium and Bayes' theorem.J Am Coll Cardiol. 2010 Aug 10;56(7):611-2; author replies 614-5. doi: 10.1016/j.jacc.2010.03.061. J Am Coll Cardiol. 2010. PMID: 20688218 No abstract available.
-
What is the real negative predictive value of a zero calcium score?J Am Coll Cardiol. 2010 Aug 10;56(7):611; author replies 614-5. doi: 10.1016/j.jacc.2010.02.062. J Am Coll Cardiol. 2010. PMID: 20688219 No abstract available.
-
What is the prognostic value of a zero calcium score? Ask Bayes!J Am Coll Cardiol. 2010 Aug 10;56(7):612; author replies 614-5. doi: 10.1016/j.jacc.2010.03.060. J Am Coll Cardiol. 2010. PMID: 20688220 No abstract available.
-
Coronary calcification and coronary artery disease.J Am Coll Cardiol. 2010 Aug 10;56(7):613; author replies 614-5. doi: 10.1016/j.jacc.2010.03.057. J Am Coll Cardiol. 2010. PMID: 20688221 No abstract available.
-
Coronary calcium remains an effective filter for invasive angiography.J Am Coll Cardiol. 2010 Aug 10;56(7):613-4; author replies 614-5. doi: 10.1016/j.jacc.2010.03.056. J Am Coll Cardiol. 2010. PMID: 20688222 No abstract available.
-
Coronary artery disease. Calcium score of zero: not a gatekeeper to rule out coronary artery disease.Rev Cardiovasc Med. 2010 Fall;11(4):271-3. doi: 10.3909/ricm0568. Rev Cardiovasc Med. 2010. PMID: 21389919 Free PMC article.
References
-
- Stary HC, Chandler AB, Dinsmore RE, et al. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. A report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Arterioscler Thromb Vasc Biol. 1995;15:1512–31. - PubMed
-
- Rumberger JA, Simons DB, Fitzpatrick LA, Sheedy PF, Schwartz RS. Coronary artery calcium area by electron-beam computed tomography and coronary atherosclerotic plaque area. A histopathologic correlative study. Circulation. 1995;92:2157–62. - PubMed
-
- Falk E, Shah PK, Fuster V. Coronary plaque disruption. Circulation. 1995;92:657–71. - PubMed
-
- Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. J Am Coll Cardiol. 2006;47:C13–8. - PubMed
-
- Greenland P, Bonow RO, Brundage BH, et al. ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) J Am Coll Cardiol. 2007;49:378–402. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
