

Increased oxidative stress and cardiomyocyte myofibrillar degeneration in patients with chronic isolated mitral regurgitation and ejection fraction >60%
- PMID: 20170794
- PMCID: PMC3092364
- DOI: 10.1016/j.jacc.2009.08.074
Increased oxidative stress and cardiomyocyte myofibrillar degeneration in patients with chronic isolated mitral regurgitation and ejection fraction >60%
Abstract
Objectives: This study assessed myocardial damage in patients with chronic isolated mitral regurgitation (MR) and left ventricular ejection fraction (LVEF) >60%.
Background: Typically, MR patients have decreased LVEF after mitral valve (MV) repair despite normal pre-operative LVEF.
Methods: Twenty-seven patients with isolated MR had left ventricular (LV) biopsies taken at time of MV repair. Magnetic resonance imaging with tissue tagging was performed in 40 normal subjects and in MR patients before and 6 months after MV repair.
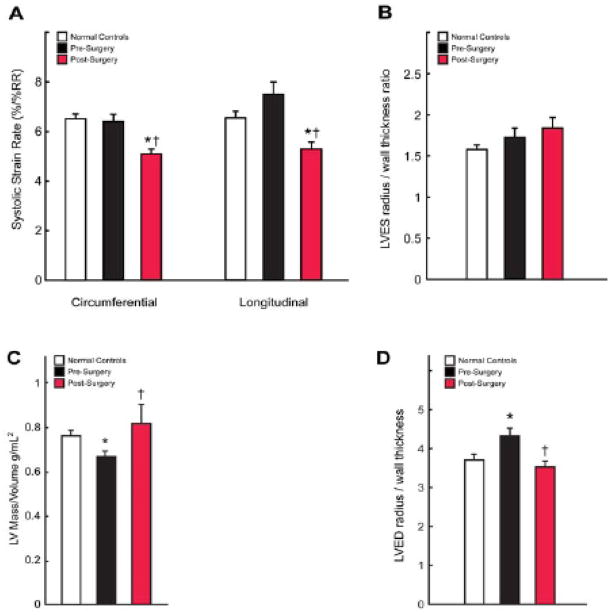
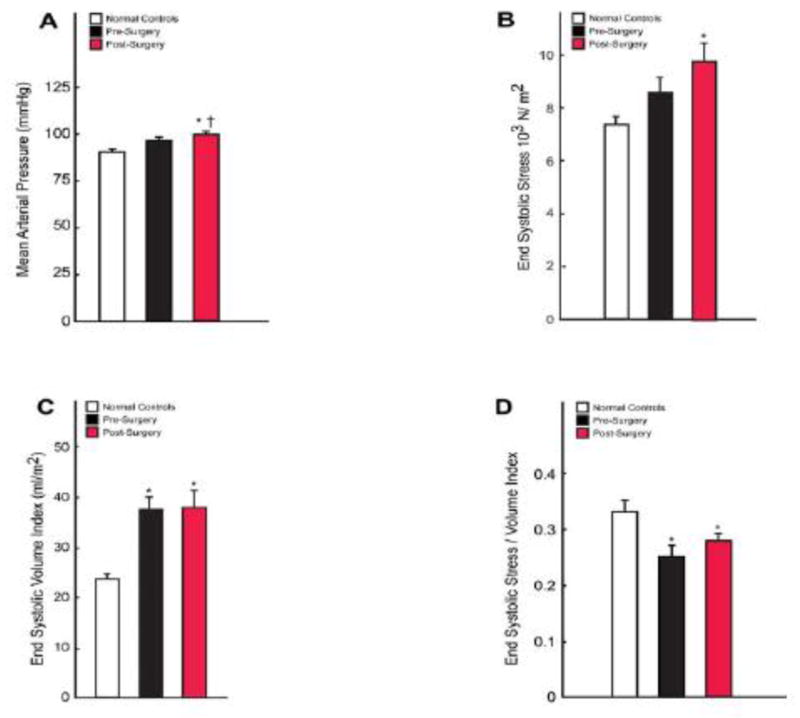
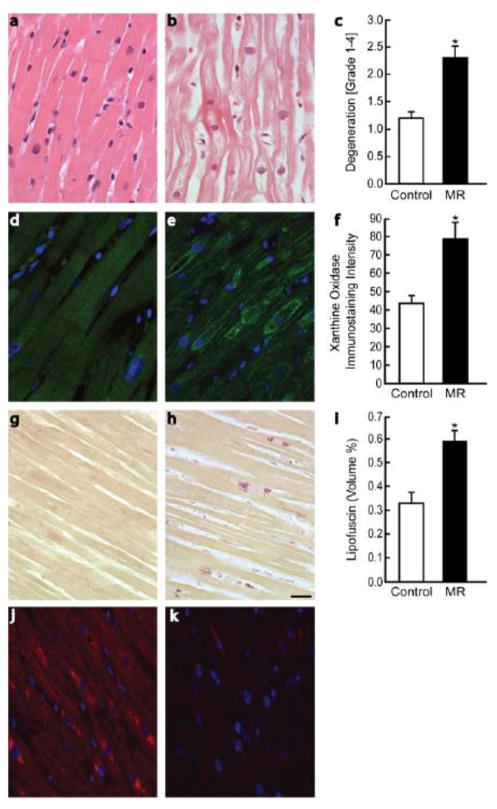
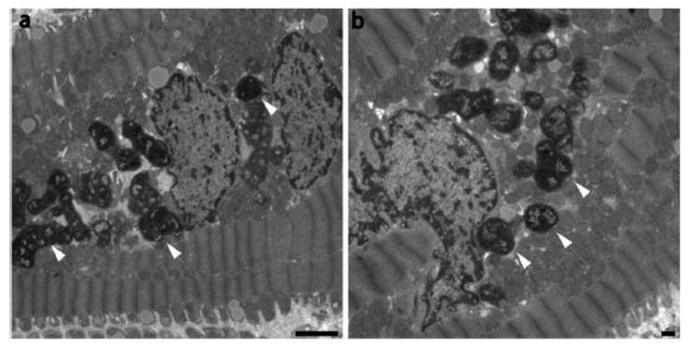
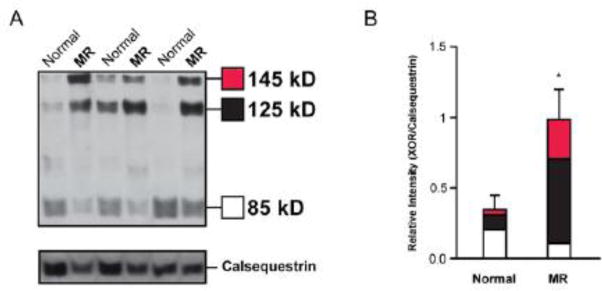
Results: LVEF (66 +/- 5% to 54 +/- 9%, p < 0.0001) and LV end-diastolic volume index (108 +/- 28 ml/m(2) to 78 +/- 24 ml/m(2), p < 0.0001) decreased, whereas left ventricular end-systolic (LVES) volume index was 60% above normal pre- and post-MV repair (p < 0.05). The LV circumferential and longitudinal strain rates decreased below normal following MV repair (6.38 +/- 1.38 vs. 5.11 +/- 1.28, p = 0.0009, and 7.51 +/- 2.58 vs. 5.31 +/- 1.61, percentage of R to R interval, p < 0.0001), as LVES stress/LVES volume index ratio was depressed at baseline and following MV repair versus normal subjects (0.25 +/- 0.10 and 0.28 +/- 0.05 vs. 0.33 +/- 0.12, p < 0.01). LV biopsies demonstrated cardiomyocyte myofibrillar degeneration versus normal subjects (p = 0.035). Immunostaining and immunoblotting demonstrated increased xanthine oxidase in MR versus normal subjects (p < 0.05). Lipofuscin deposition was increased in cardiomyocytes of MR versus normal subjects (0.62 +/- 0.20 vs. 0.33 +/- 0.11, percentage of area: p < 0.01).
Conclusions: Decreased LV strain rates and LVES wall stress/LVES volume index following MV repair indicate contractile dysfunction, despite pre-surgical LVEF >60%. Increased oxidative stress could cause myofibrillar degeneration and lipofuscin accumulation resulting in LV contractile dysfunction in MR.
Figures
References
-
- Borer JS, Bonow RO. Contemporary approach to aortic and mitral regurgitation. Circulation. 2003;108:2432–8. - PubMed
-
- Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48:e1–148. - PubMed
-
- Le Tourneau T, de Groote P, Millaire A, et al. Effect of mitral valve surgery on exercise capacity, ventricular ejection fraction and neurohormonal activation in patients with severe mitral regurgitation. J Am Coll Cardiol. 2000;36:2263–9. - PubMed
-
- Madaric J, Watripont P, Bartunek J, et al. Effect of mitral valve repair on exercise tolerance in asymptomatic patients with organic mitral regurgitation. Am Heart J. 2007;154:180–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
