

Outcome from a randomized controlled trial of group therapy for binge eating disorder: comparing dialectical behavior therapy adapted for binge eating to an active comparison group therapy
- PMID: 20171332
- PMCID: PMC3170852
- DOI: 10.1016/j.beth.2009.01.006
Outcome from a randomized controlled trial of group therapy for binge eating disorder: comparing dialectical behavior therapy adapted for binge eating to an active comparison group therapy
Erratum in
- Behav Ther. 2010 Sep;41(3):432. Robinson, Athena Hagler [added]
Abstract
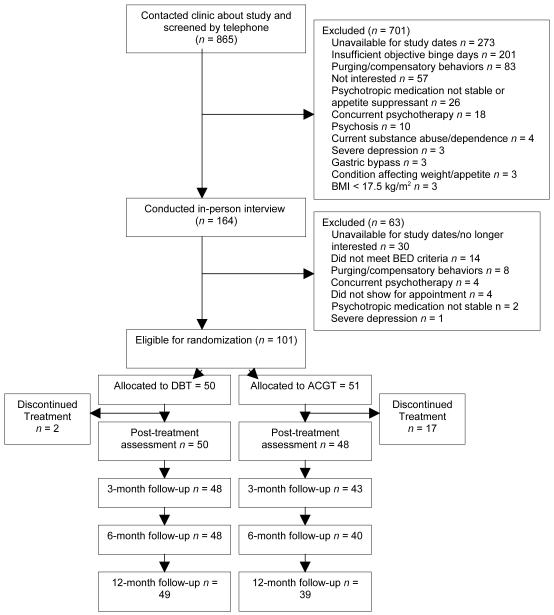
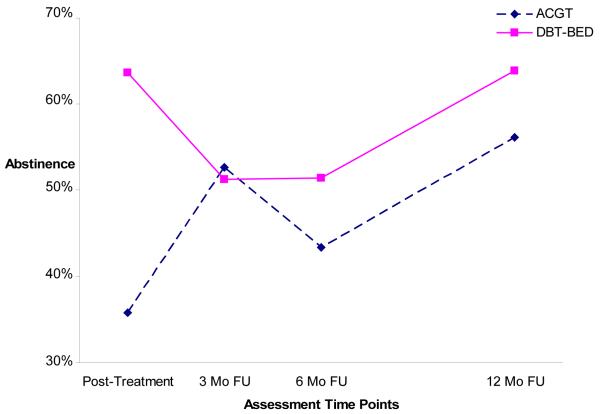
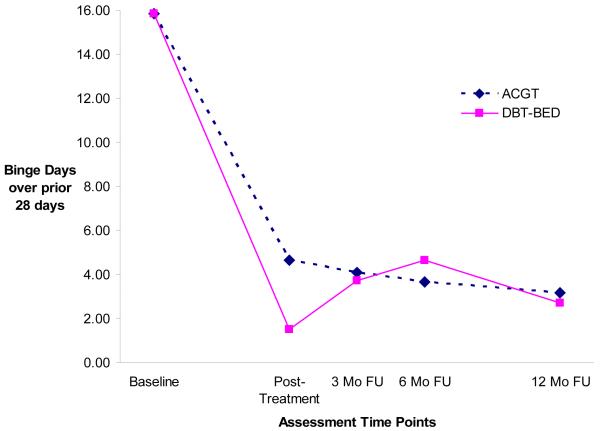
Dialectical Behavior Therapy for Binge Eating Disorder (DBT-BED) aims to reduce binge eating by improving adaptive emotion-regulation skills. Preliminary findings have been promising but have only compared DBT-BED to a wait-list. To control for the hypothesized specific effects of DBT-BED, the present study compared DBT-BED to an active comparison group therapy (ACGT). Men and women (n=101) meeting DSM-IV BED research criteria were randomly assigned to 20 group sessions of DBT-BED (n=50) or ACGT (n=51). DBT-BED had a significantly lower dropout rate (4%) than ACGT (33.3%). Linear Mixed Models revealed that posttreatment binge abstinence and reductions in binge frequency were achieved more quickly for DBT-BED than for ACGT (posttreatment abstinence rate=64% for DBT-BED vs. 36% for ACGT) though differences did not persist over the 3-, 6-, and 12-month follow-up assessments (e.g., 12-month follow-up abstinence rate=64% for DBT-BED vs. 56% for ACGT). Secondary outcome measures revealed no sustained impact on emotion regulation. Although both DBT-BED and ACGT reduced binge eating, DBT-BED showed significantly fewer dropouts and greater initial efficacy (e.g., at posttreatment) than ACGT. The lack of differential findings over follow-up suggests that the hypothesized specific effects of DBT-BED do not show long-term impact beyond those attributable to nonspecific common therapeutic factors.
2010. Published by Elsevier Ltd.
Figures
Similar articles
-
Does rapid response to two group psychotherapies for binge eating disorder predict abstinence?Behav Res Ther. 2011 May;49(5):339-45. doi: 10.1016/j.brat.2011.03.001. Epub 2011 Mar 16. Behav Res Ther. 2011. PMID: 21459363 Free PMC article. Clinical Trial.
-
Treatment of binge eating disorder.Psychiatr Clin North Am. 2011 Dec;34(4):773-83. doi: 10.1016/j.psc.2011.08.011. Epub 2011 Oct 5. Psychiatr Clin North Am. 2011. PMID: 22098803
-
Moderators of dialectical behavior therapy for binge eating disorder: results from a randomized controlled trial.Int J Eat Disord. 2012 May;45(4):597-602. doi: 10.1002/eat.20932. Epub 2011 Apr 15. Int J Eat Disord. 2012. PMID: 21500238 Free PMC article. Clinical Trial.
-
Rates of abstinence following psychological or behavioral treatments for binge-eating disorder: Meta-analysis.Int J Eat Disord. 2018 Aug;51(8):785-797. doi: 10.1002/eat.22897. Epub 2018 Jul 29. Int J Eat Disord. 2018. PMID: 30058074 Review.
-
Psychological treatments for binge eating disorder.Curr Psychiatry Rep. 2012 Aug;14(4):432-46. doi: 10.1007/s11920-012-0277-8. Curr Psychiatry Rep. 2012. PMID: 22707016 Free PMC article. Review.
Cited by
-
A Qualitative Assessment of the Parenting Challenges and Treatment Needs of Mothers with Borderline Personality Disorder.J Psychother Integr. 2015 Jun 1;25(2):71-89. doi: 10.1037/a0038877. J Psychother Integr. 2015. PMID: 26257507 Free PMC article.
-
Dialectical behavior therapy adapted for binge eating compared to cognitive behavior therapy in obese adults with binge eating disorder: a controlled study.J Eat Disord. 2020 Jun 10;8(1):27. doi: 10.1186/s40337-020-00299-z. eCollection 2020. J Eat Disord. 2020. PMID: 32528681 Free PMC article.
-
The feasibility of emotion-focused therapy for binge-eating disorder: a pilot randomised wait-list control trial.J Eat Disord. 2021 Jan 6;9(1):2. doi: 10.1186/s40337-020-00358-5. J Eat Disord. 2021. PMID: 33407948 Free PMC article.
-
"I mean, it kind of saved my life, to be honest": a qualitative study of participants' views of a dialectical behaviour therapy for multidiagnostic eating disorders programme.J Eat Disord. 2024 Nov 20;12(1):186. doi: 10.1186/s40337-024-01142-5. J Eat Disord. 2024. PMID: 39567973 Free PMC article.
-
Dialectical behavior therapy for adolescents: theory, treatment adaptations, and empirical outcomes.Clin Child Fam Psychol Rev. 2013 Mar;16(1):59-80. doi: 10.1007/s10567-012-0126-7. Clin Child Fam Psychol Rev. 2013. PMID: 23224757 Review.
References
-
- Abraham SF, Beumont PJ. How patients describe bulimia or binge eating. Psychological Medicine. 1982;12:625–635. - PubMed
-
- Agras WS, Walsh T, Fairburn CG, Wilson GT, Kraemer HC. A multicenter comparison of cognitive-behavioral therapy and interpersonal psychotherapy for bulimia nervosa. Archives of General Psychiatry. 2000;57:459–66. - PubMed
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 4th ed Author; Washington, DC: 1994.
-
- American Psychiatric Association Practice guideline for the treatment of patients with borderline personality disorders. American Journal of Psychiatry. 2001;168:1–52. - PubMed
-
- Arnow B, Kenardy J, Agras WS. Binge eating among the obese: A descriptive study. Journal of Behavioral Medicine. 1992;15:155–170. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
