

Radiotherapy dose-volume effects on salivary gland function
- PMID: 20171519
- PMCID: PMC4041494
- DOI: 10.1016/j.ijrobp.2009.06.090
Radiotherapy dose-volume effects on salivary gland function
Abstract
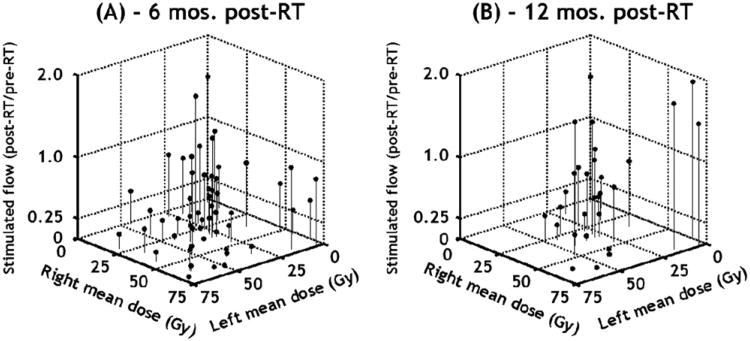
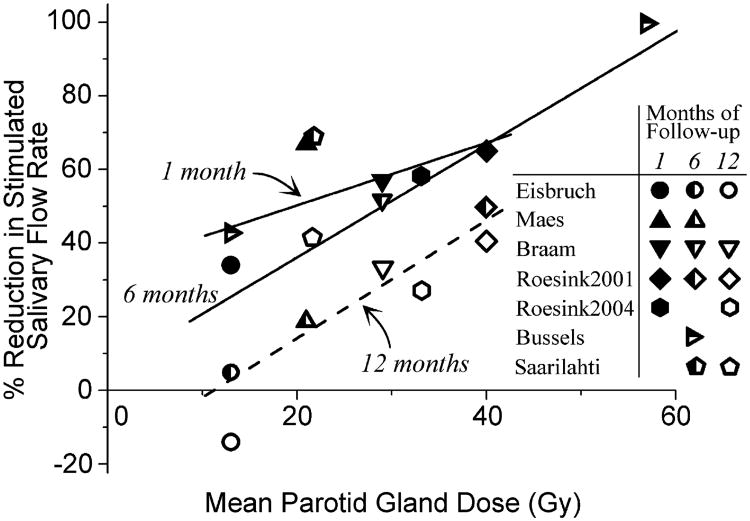
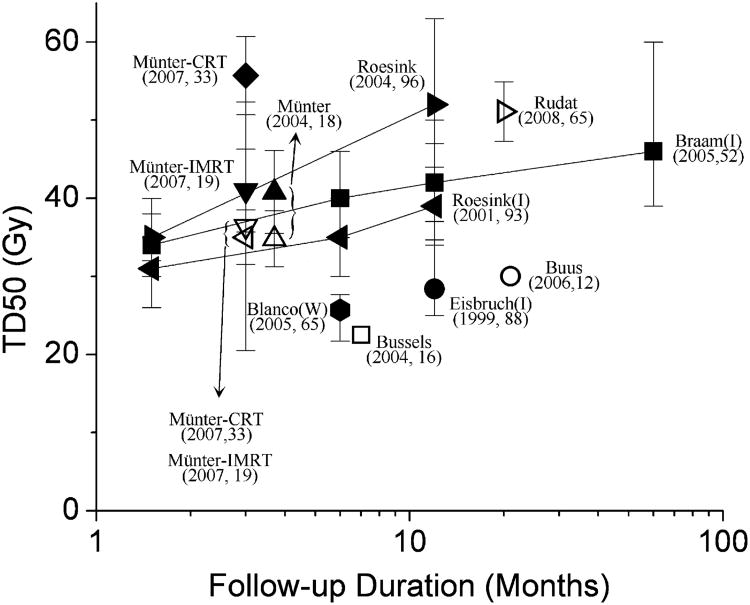
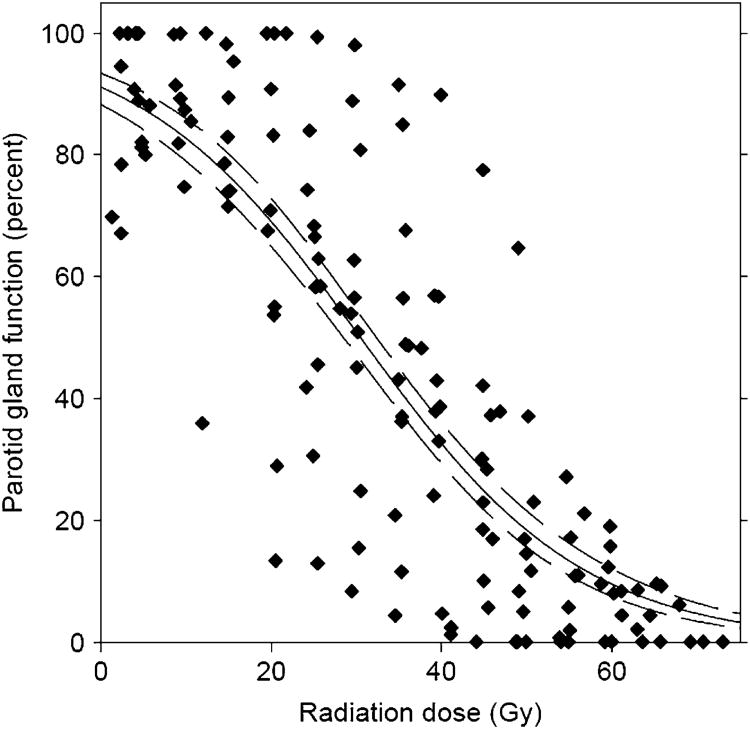
Publications relating parotid dose-volume characteristics to radiotherapy-induced salivary toxicity were reviewed. Late salivary dysfunction has been correlated to the mean parotid gland dose, with recovery occurring with time. Severe xerostomia (defined as long-term salivary function of <25% of baseline) is usually avoided if at least one parotid gland is spared to a mean dose of less than approximately 20 Gy or if both glands are spared to less than approximately 25 Gy (mean dose). For complex, partial-volume RT patterns (e.g., intensity-modulated radiotherapy), each parotid mean dose should be kept as low as possible, consistent with the desired clinical target volume coverage. A lower parotid mean dose usually results in better function. Submandibular gland sparing also significantly decreases the risk of xerostomia. The currently available predictive models are imprecise, and additional study is required to identify more accurate models of xerostomia risk.
Copyright 2010 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: none.
Figures
Similar articles
-
Using a reduced spot size for intensity-modulated proton therapy potentially improves salivary gland-sparing in oropharyngeal cancer.Int J Radiat Oncol Biol Phys. 2012 Feb 1;82(2):e313-9. doi: 10.1016/j.ijrobp.2011.05.005. Epub 2011 Jun 25. Int J Radiat Oncol Biol Phys. 2012. PMID: 21708427
-
A phase II study to assess the efficacy of amifostine for submandibular/sublingual salivary sparing during the treatment of head and neck cancer with intensity modulated radiation therapy for parotid salivary sparing.Semin Oncol. 2004 Dec;31(6 Suppl 18):25-8. doi: 10.1053/j.seminoncol.2004.12.008. Semin Oncol. 2004. PMID: 15726519 Clinical Trial.
-
Impact of salivary gland dosimetry on post-IMRT recovery of saliva output and xerostomia grade for head-and-neck cancer patients treated with or without contralateral submandibular gland sparing: a longitudinal study.Int J Radiat Oncol Biol Phys. 2011 Dec 1;81(5):1479-87. doi: 10.1016/j.ijrobp.2010.07.1990. Epub 2010 Oct 8. Int J Radiat Oncol Biol Phys. 2011. PMID: 20934262
-
Dose and volume impact on radiation-induced xerostomia.Rays. 2005 Apr-Jun;30(2):145-8. Rays. 2005. PMID: 16294907 Review.
-
Prospective investigation and literature review of tolerance dose on salivary glands using quantitative salivary gland scintigraphy in the intensity-modulated radiotherapy era.Head Neck. 2016 Apr;38 Suppl 1:E1746-55. doi: 10.1002/hed.24310. Epub 2016 Feb 15. Head Neck. 2016. PMID: 26875880 Review.
Cited by
-
The clinical case for proton beam therapy.Radiat Oncol. 2012 Oct 22;7:174. doi: 10.1186/1748-717X-7-174. Radiat Oncol. 2012. PMID: 23083010 Free PMC article. Review.
-
Modeling of Xerostomia After Radiotherapy for Head and Neck Cancer: A Registry Study.Front Oncol. 2020 Aug 14;10:1647. doi: 10.3389/fonc.2020.01647. eCollection 2020. Front Oncol. 2020. PMID: 32923404 Free PMC article.
-
Unilateral neck therapy in the human papillomavirus ERA: accepted regional spread patterns.Head Neck. 2013 Feb;35(2):160-4. doi: 10.1002/hed.22929. Epub 2012 Feb 2. Head Neck. 2013. PMID: 22302641 Free PMC article.
-
Head and neck region consolidation radiotherapy and prophylactic cranial irradiation with hippocampal avoidance delivered with helical tomotherapy after induction chemotherapy for non-sinonasal neuroendocrine carcinoma of the upper airways.Radiat Oncol. 2012 Feb 15;7:21. doi: 10.1186/1748-717X-7-21. Radiat Oncol. 2012. PMID: 22336394 Free PMC article.
-
MR-Guided Adaptive Radiotherapy for OAR Sparing in Head and Neck Cancers.Cancers (Basel). 2022 Apr 10;14(8):1909. doi: 10.3390/cancers14081909. Cancers (Basel). 2022. PMID: 35454816 Free PMC article. Review.
References
-
- Dawes C, Wood CM. The contribution of oral minor mucous gland secretions to the volume of whole saliva in man. Arch Oral Biol. 1973;18:337–342. - PubMed
-
- Buus S, Grau C, Munk O, et al. Individual radiation response of parotid glands investigated by dynamic 11C-methionine PET. Radiother Oncol. 2006;78:262–269. - PubMed
-
- Astreinidou E, Roesink JM, Raaijmakers CP, et al. 3D MR sialography as a tool to investigate radiation-induced xerostomia: Feasibility study. Int J Radiat Oncol Biol Phys. 2007;68:1310–1319. - PubMed
-
- Chao KSC, Deasy JO, Markman J, et al. A prospective study of salivary function sparing in patients with head-and-neck cancers receiving intensity-modulated or three-dimensional radiation therapy: Initial results. Int J Radiat Oncol Biol Phys. 2001;49:907–916. - PubMed
-
- Meirovitz A, Murdoch-Kinch C, Schipper M, et al. Grading xerostomia by physicians or by patients after intensity-modulated radiotherapy of head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2006;66:445–453. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
