

The learning curve for surgical margins after open radical prostatectomy: implications for margin status as an oncological end point
- PMID: 20171687
- PMCID: PMC2861336
- DOI: 10.1016/j.juro.2009.12.015
The learning curve for surgical margins after open radical prostatectomy: implications for margin status as an oncological end point
Abstract
Purpose: Surgical margin status is commonly used as an end point for surgical learning. We examined the surgical margin learning curve and investigated whether surgical margins are a good marker for oncological outcome.
Materials and methods: The study cohort included 7,765 patients with prostate cancer treated with radical prostatectomy by 1 of 72 surgeons at a total of 4 major American academic medical centers. We calculated the learning curve for surgical margins and a concordance probability between the surgeon rates of positive surgical margins and 5-year biochemical recurrence.
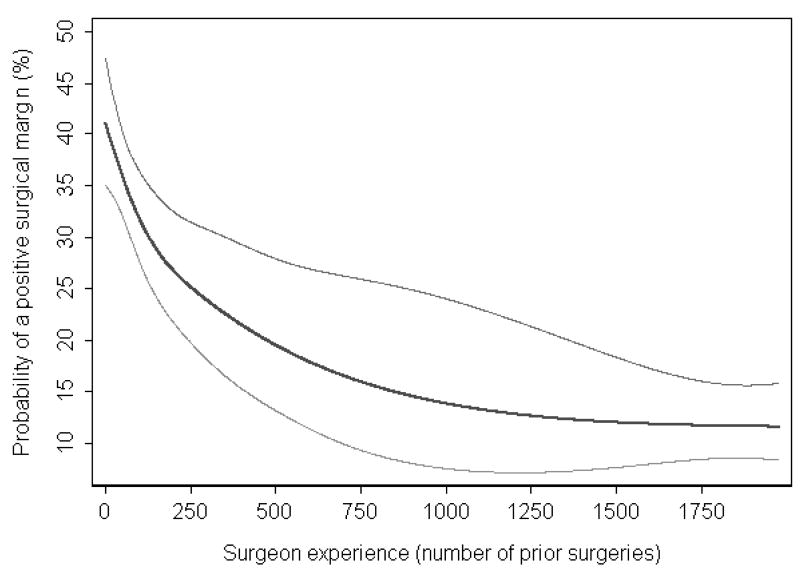
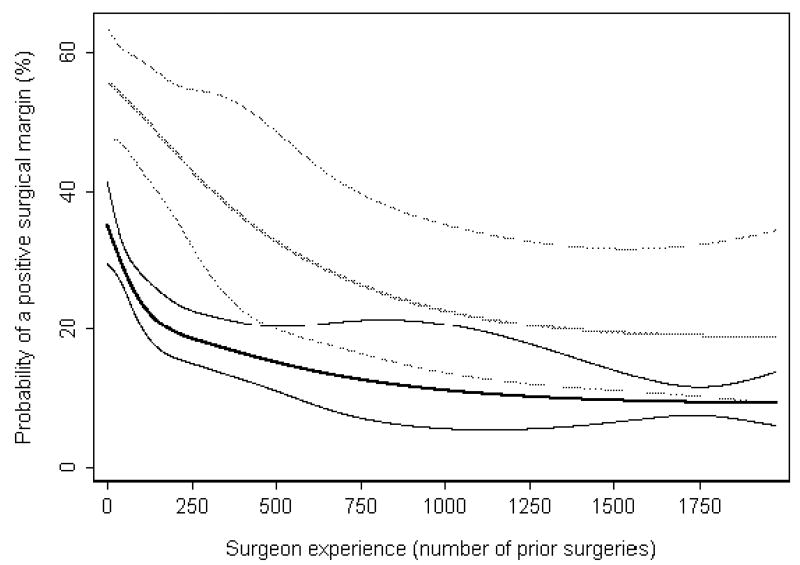
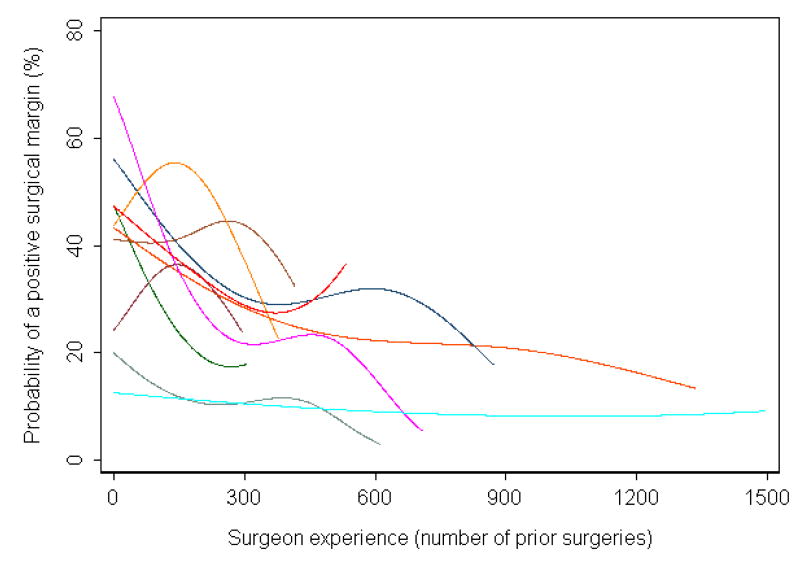
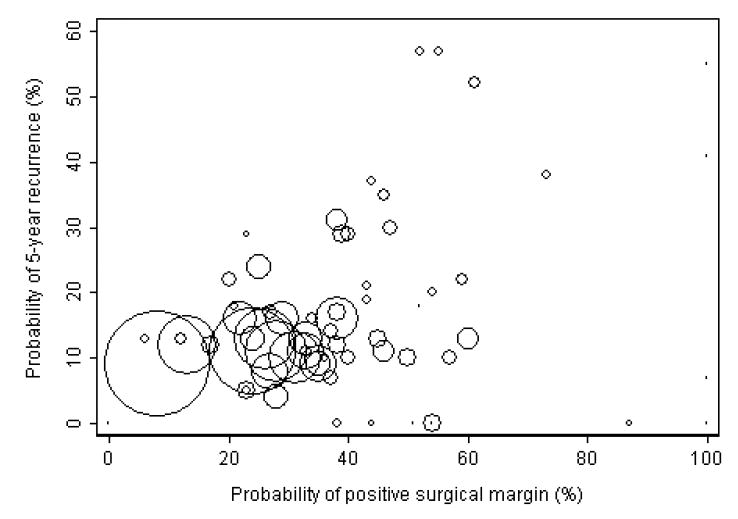
Results: A positive surgical margin was identified in 2,059 patients (27%). On multivariate analysis surgeon experience was strongly associated with surgical margin status (p = 0.017). The probability of a positive surgical margin was 40% for a surgeon with 10 prior cases, which decreased to 25% for a surgeon with 250 (absolute difference 15%, 95% CI 11 to 18). Learning curves differed dramatically among surgeons. For surgeon pairs the surgeon with the superior positive surgical margin rate also had the better biochemical recurrence rate only 58% of the time.
Conclusions: We noted a learning curve for surgical margins after open radical prostatectomy. The poor concordance between surgeon margin and recurrence rates suggests that while margins clearly matter and efforts should be made to decrease positive margin rates, surgical margin status is not a strong surrogate for cancer control. These results have implications for using the margin rate to evaluate changes in surgical technique and as surgeon feedback.
Copyright (c) 2010 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Editorial comment.J Urol. 2010 Apr;183(4):1365. doi: 10.1016/j.juro.2009.12.120. Epub 2010 Feb 19. J Urol. 2010. PMID: 20171674 No abstract available.
-
Words of Wisdom. Re: the learning curve for surgical margins after open radical prostatectomy: implications for the use of margin status as an oncologic endpoint.Eur Urol. 2011 Jan;59(1):171-2. doi: 10.1016/j.eururo.2010.10.014. Eur Urol. 2011. PMID: 21414872 No abstract available.
References
-
- Vickers AJ, Bianco FJ, Serio AM, et al. The surgical learning curve for prostate cancer control after radical prostatectomy. J Natl Cancer Inst. 2007;99:1171. - PubMed
-
- Eggleston JC, Walsh PC. Radical prostatectomy with preservation of sexual function: pathological findings in the first 100 cases. J Urol. 1985;134:1146. - PubMed
-
- Kaul S, Savera A, Badani K, et al. Functional outcomes and oncological efficacy of Vattikuti Institute prostatectomy with Veil of Aphrodite nerve-sparing: an analysis of 154 consecutive patients. BJU Int. 2006;97:467. - PubMed
-
- Ruiz L, Salomon L, Hoznek A, et al. Comparison of early oncologic results of laparoscopic radical prostatectomy by extraperitoneal versus transperitoneal approach. Eur Urol. 2004;46:50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
