

Prospective imaging assessment of mortality risk after head-and-neck radiotherapy
- PMID: 20171802
- PMCID: PMC3072063
- DOI: 10.1016/j.ijrobp.2009.08.063
Prospective imaging assessment of mortality risk after head-and-neck radiotherapy
Abstract
Purpose: The optimal roles for imaging-based biomarkers in the management of head-and-neck cancer remain undefined. Unresolved questions include whether functional or anatomic imaging might improve mortality risk assessment for this disease. We addressed these issues in a prospective institutional trial.
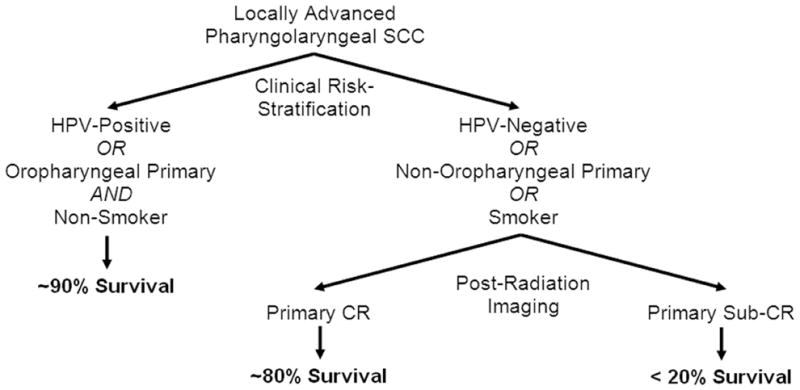
Methods and materials: Ninety-eight patients with locally advanced pharyngolaryngeal squamous cell cancer were enrolled. Each underwent pre- and post-chemoradiotherapy contrast-enhanced computed tomography (CT) and (18)F-fluorodeoxyglucose (FDG)-positron emission tomography (PET)/CT imaging. Imaging parameters were correlated with survival outcomes.
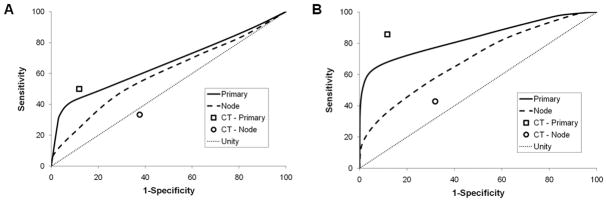
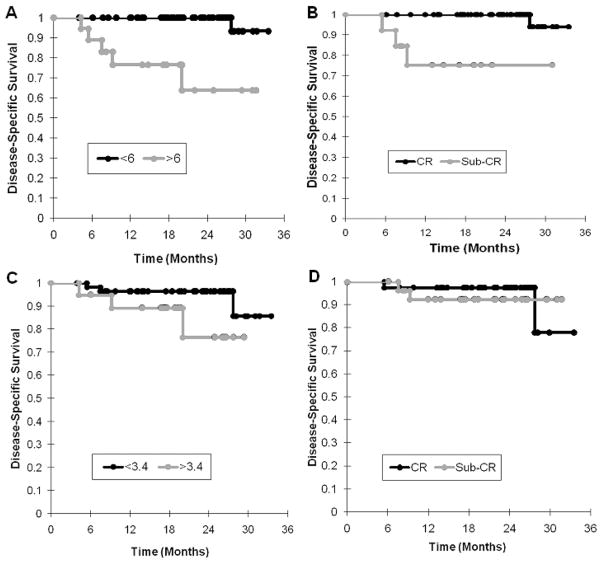
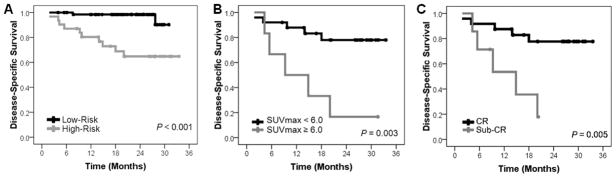
Results: Low post-radiation primary tumor FDG avidity correlated with improved survival on multivariate analysis; so too did complete primary tumor response by CT alone. Although both imaging modalities lacked sensitivity, each had high specificity and negative predictive value for disease-specific mortality risk assessment. Kaplan-Meier estimates confirmed that both CT and FDG-PET/CT stratify patients into distinct high- and low-probability survivorship groups on the basis of primary tumor response to radiotherapy. Subset analyses demonstrated that the prognostic value for each imaging modality was primarily derived from patients at high risk for local treatment failure (human papillomavirus [HPV]-negative disease, nonoropharyngeal primary disease, or tobacco use).
Conclusions: CT alone and FDG-PET/CT are potentially useful tools in head-and-neck cancer-specific mortality risk assessment after radiotherapy, particularly for selective use in cases of high-risk HPV-unrelated disease. Focus should be placed on corroboration and refinement of patient selection for imaging-based biomarkers in future studies.
Copyright © 2010 Elsevier Inc. All rights reserved.
Conflict of interest statement
None exist.
Figures
Similar articles
-
Prospective risk-adjusted [18F]Fluorodeoxyglucose positron emission tomography and computed tomography assessment of radiation response in head and neck cancer.J Clin Oncol. 2009 May 20;27(15):2509-15. doi: 10.1200/JCO.2008.19.3300. Epub 2009 Mar 30. J Clin Oncol. 2009. PMID: 19332725 Free PMC article. Clinical Trial.
-
Change of maximum standardized uptake value slope in dynamic triphasic [18F]-fluorodeoxyglucose positron emission tomography/computed tomography distinguishes malignancy from postradiation inflammation in head-and-neck squamous cell carcinoma: a prospective trial.Int J Radiat Oncol Biol Phys. 2015 Mar 1;91(3):472-9. doi: 10.1016/j.ijrobp.2014.11.002. Epub 2015 Jan 30. Int J Radiat Oncol Biol Phys. 2015. PMID: 25680593 Free PMC article.
-
Assessment of outcomes with delayed (18)F-FDG PET-CT response assessment in head and neck squamous cell carcinoma.Br J Radiol. 2015 Aug;88(1052):20140592. doi: 10.1259/bjr.20140592. Epub 2015 Jun 17. Br J Radiol. 2015. PMID: 26081447 Free PMC article.
-
Update on 18F-fluorodeoxyglucose/positron emission tomography and positron emission tomography/computed tomography imaging of squamous head and neck cancers.Semin Nucl Med. 2005 Oct;35(4):214-9. doi: 10.1053/j.semnuclmed.2005.05.001. Semin Nucl Med. 2005. PMID: 16150243 Review.
-
FDG-PET/CT for treatment response assessment in head and neck squamous cell carcinoma: a systematic review and meta-analysis of diagnostic performance.Eur J Nucl Med Mol Imaging. 2018 Jun;45(6):1063-1071. doi: 10.1007/s00259-018-3978-3. Epub 2018 Feb 24. Eur J Nucl Med Mol Imaging. 2018. PMID: 29478080
Cited by
-
Functional imaging in radiation therapy planning for head and neck cancer.Rep Pract Oncol Radiother. 2013 Nov 9;18(6):376-82. doi: 10.1016/j.rpor.2013.10.007. Rep Pract Oncol Radiother. 2013. PMID: 24416582 Free PMC article. Review.
-
Post-radiotherapy PET/CT for predicting treatment outcomes in head and neck cancer after postoperative radiotherapy.Eur J Nucl Med Mol Imaging. 2019 Apr;46(4):794-800. doi: 10.1007/s00259-019-4272-8. Epub 2019 Jan 24. Eur J Nucl Med Mol Imaging. 2019. PMID: 30680587
-
Metabolic tumor volume as a prognostic imaging-based biomarker for head-and-neck cancer: pilot results from Radiation Therapy Oncology Group protocol 0522.Int J Radiat Oncol Biol Phys. 2015 Mar 15;91(4):721-9. doi: 10.1016/j.ijrobp.2014.12.023. Int J Radiat Oncol Biol Phys. 2015. PMID: 25752384 Free PMC article.
-
Application of fluorodeoxyglucose positron emission tomography in the management of head and neck cancers.World J Radiol. 2014 Jun 28;6(6):238-51. doi: 10.4329/wjr.v6.i6.238. World J Radiol. 2014. PMID: 24976927 Free PMC article. Review.
-
Metabolic imaging biomarkers of postradiotherapy xerostomia.Int J Radiat Oncol Biol Phys. 2012 Aug 1;83(5):1609-16. doi: 10.1016/j.ijrobp.2011.10.074. Epub 2012 May 30. Int J Radiat Oncol Biol Phys. 2012. PMID: 22658215 Free PMC article.
References
-
- Denis F, Garaud P, Bardet E, et al. Final results of the 94-01 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. J Clin Oncol. 2004;22:69–76. - PubMed
-
- Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med. 2006;354:567–578. - PubMed
-
- Jeremic B, Shibamoto Y, Milicic B, et al. Hyperfractionated radiation therapy with or without concurrent low-dose daily cisplatin in locally advanced squamous cell carcinoma of the head and neck: a prospective randomized trial. J Clin Oncol. 2000;18:1458–1464. - PubMed
-
- Yao M, Smith RB, Hoffman HT, et al. Clinical significance of postradiotherapy [18F]-fluorodeoxyglucose positron emission tomography imaging in management of head-and-neck cancer-a long-term outcome report. Int J Radiat Oncol Biol Phys. 2009;74:9–14. - PubMed
-
- Connell CA, Corry J, Milner AD, et al. Clinical impact of, and prognostic stratification by, F-18 FDG PET/CT in head and neck mucosal squamous cell carcinoma. Head Neck. 2007;29:986–995. - PubMed
