

Viral retinitis after intravitreal triamcinolone injection in patients with predisposing medical comorbidities
- PMID: 20172069
- PMCID: PMC2905234
- DOI: 10.1016/j.ajo.2009.10.019
Viral retinitis after intravitreal triamcinolone injection in patients with predisposing medical comorbidities
Abstract
Purpose: To review the cases of viral retinitis after intravitreal steroid administration at a single center, to estimate the incidence, and to propose risk factors for its occurrence.
Design: Retrospective, observational case series.
Methods: Seven hundred thirty-six intravitreal triamcinolone (IVTA) injections were administered in the clinic and operating room by 3 retina specialists at a single academic medical center between September 2002 and November 2008. Inclusion criteria were simply a history of 1 or more IVTA injections during the period. The overall incidence of viral retinitis after IVTA injection was calculated. Subsequently, a chart audit was performed to estimate the number of patients with immune-altering conditions who had received IVTA during the period, and the incidence within this subgroup was calculated.
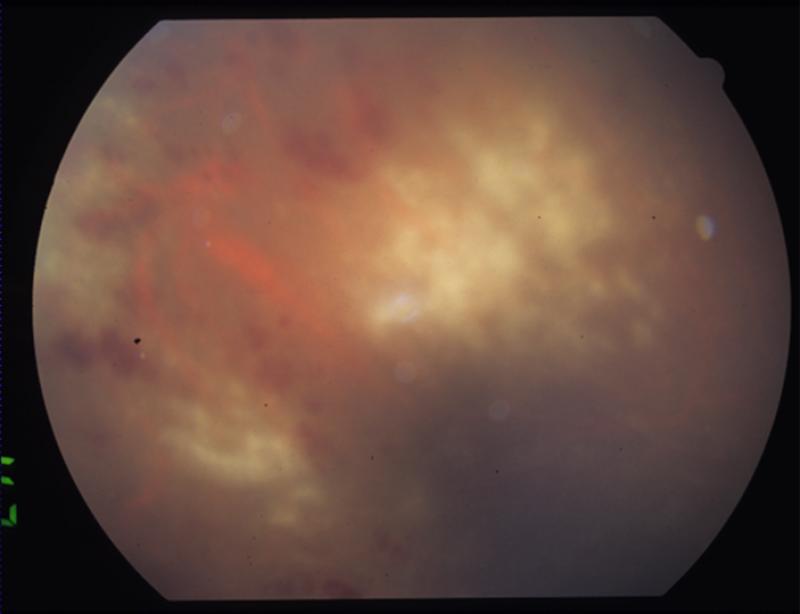
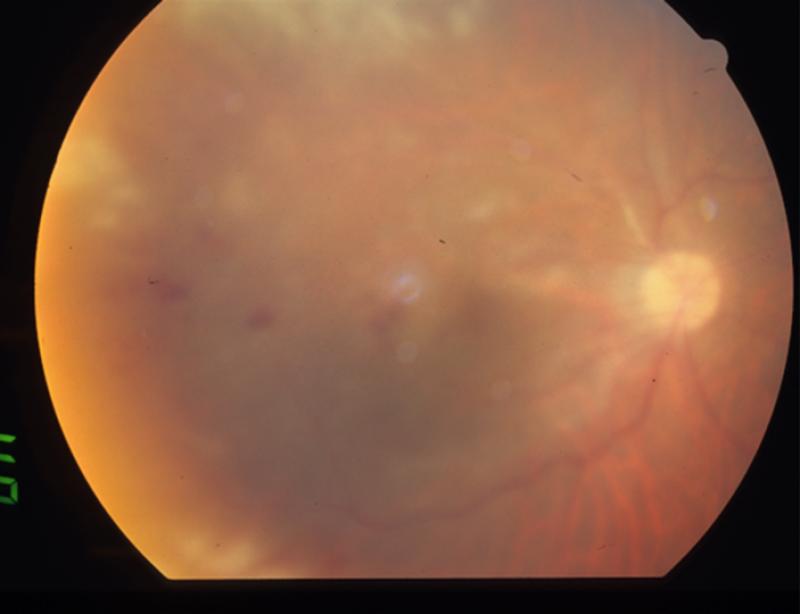
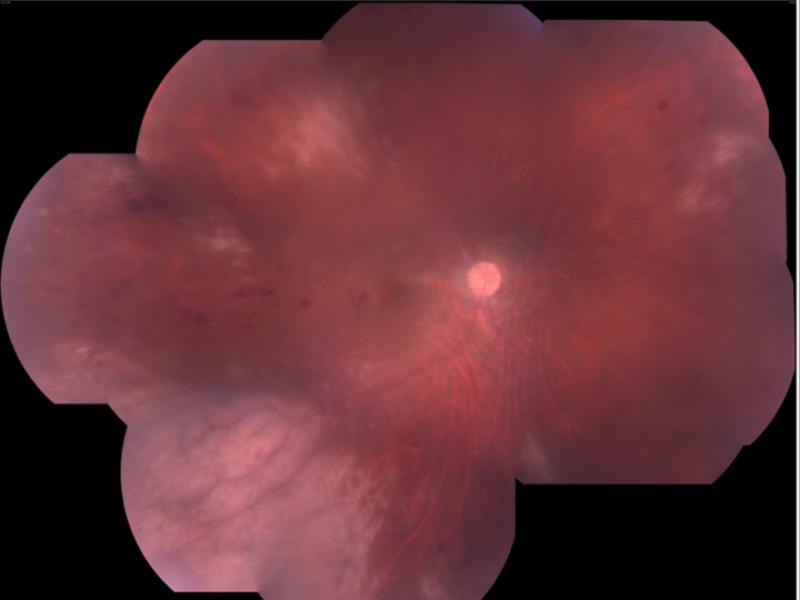
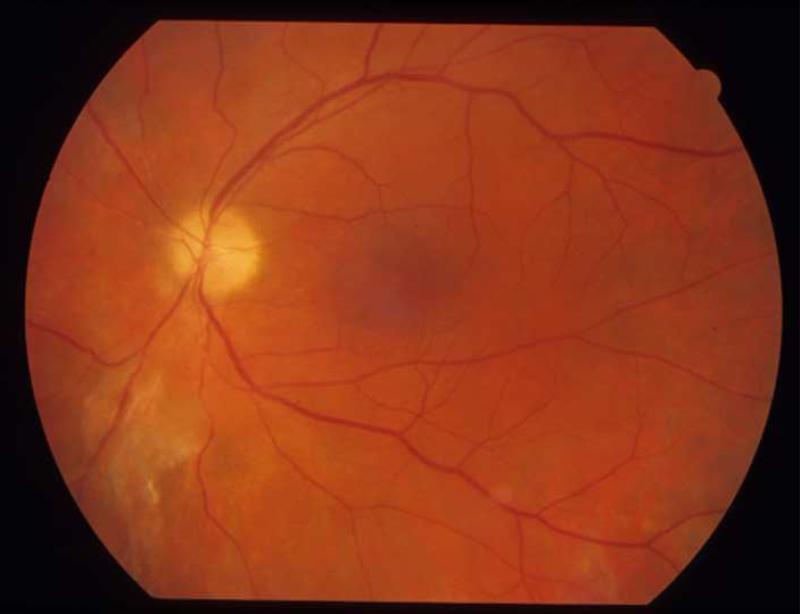
Results: Viral retinitis developed after IVTA injection in 3 patients, yielding an overall incidence of 3 in 736 or 0.41%. An estimated 334 injections were administered to patients with an immune-altering condition, including diabetes. All 3 of the patients in whom viral retinitis developed after IVTA injection possessed abnormal immune systems, yielding an incidence rate of 3 in 334 or 0.90% within this subgroup.
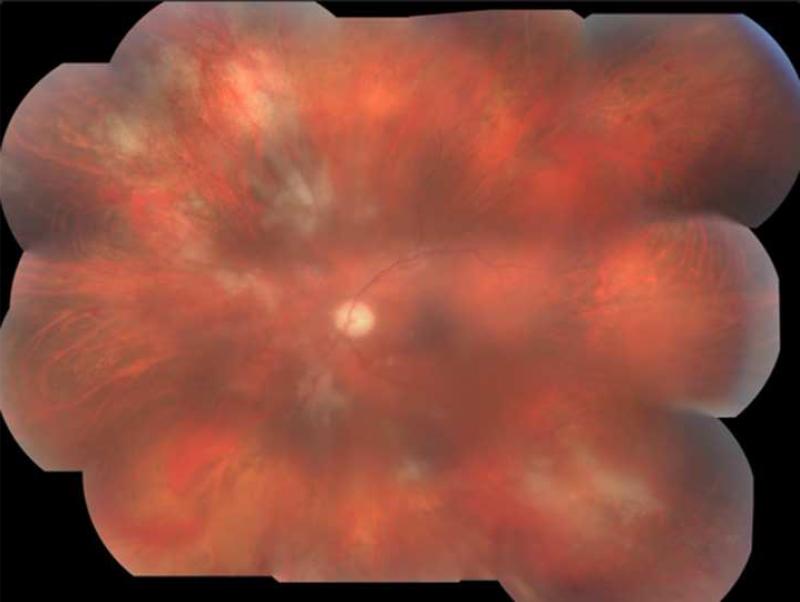
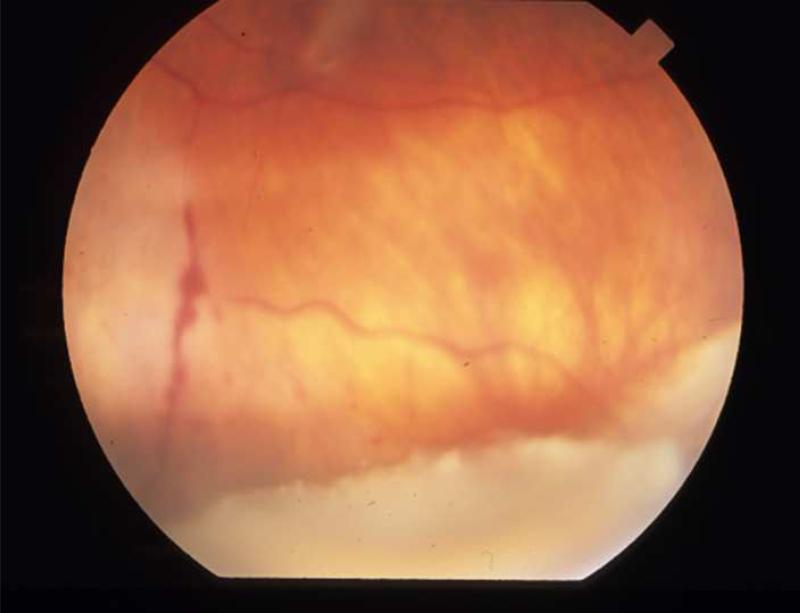
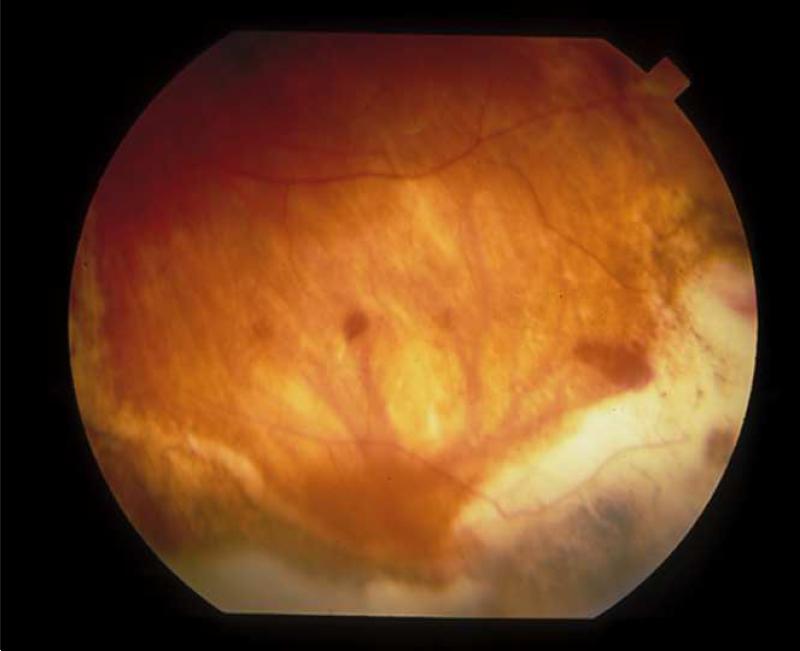
Conclusions: Our high reported incidence for this potentially devastating complication can be attributed to multiple factors, including coexisting medical immunocompromising comorbidities, a higher dose with a longer duration of local immunosuppression in the vitreous, multiple injections, as well as previous viral retinitis. Caution with a high index of clinical suspicion and frequent follow-up is advised in patients receiving IVTA injection with potentially immune-altering conditions, even after apparent immune recovery.
(c) 2010 Elsevier Inc. All rights reserved.
Figures
References
-
- Wiegand TW, Young LH. Cytomegalovirus retinitis. Int Ophthalmol Clin. 2006;46:91–110. - PubMed
-
- Kuo IC, Kempen JH, Dunn JP, et al. Clinical characteristics and outcomes of cytomegalovirus retinitis in persons without human immunodeficiency virus infection. Am J Ophthalmol. 2004;138:338–46. - PubMed
-
- Crippa F, Corey L, Chuang EL, et al. Virological, clinical, and ophthalmologic features of cytomegalovirus retinitis after hematopoietic stem cell transplantation. Clin Infect Dis. 2001;32:214–9. - PubMed
-
- Benz MS, Glaser JS, Davis JL. Progressive outer retinal necrosis in immunocompetent patients treated initially for optic neuropathy with systemic corticosteroids. Am J Ophthalmol. 2003;135:551–3. - PubMed
-
- Browning DJ. Acute retinal necrosis following epidural steroid injections. Am J Ophthalmol. 2003;136:192–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
