

Major infection after pediatric cardiac surgery: a risk estimation model
- PMID: 20172141
- PMCID: PMC3319976
- DOI: 10.1016/j.athoracsur.2009.11.048
Major infection after pediatric cardiac surgery: a risk estimation model
Abstract
Background: In pediatric cardiac surgery, infection is a leading cause of morbidity and mortality. We created a model to predict risk of major infection in this population.
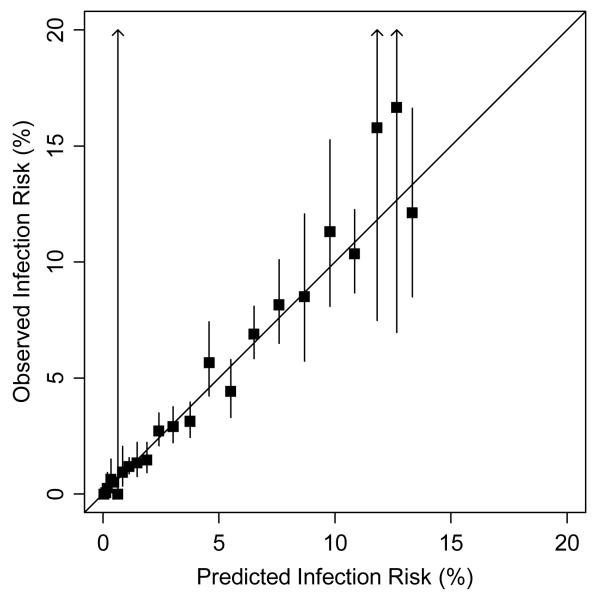
Methods: Using the Society of Thoracic Surgeons Congenital Heart Surgery Database, we created a multivariable model in which the primary outcome was major infection (septicemia, mediastinitis, or endocarditis). Candidate-independent variables included demographic characteristics, comorbid conditions, preoperative factors, and cardiac surgical procedures. We created a reduced model by backward selection and then created an integer scoring system using a scaling factor with scores corresponding to percent risk of infection.
Results: Of 30,078 children from 48 centers, 2.8% had major infection (2.6% septicemia, 0.3% mediastinitis, and 0.09% endocarditis). Mortality and postoperative length of stay were greater in those with major infection (mortality, 22.2% versus 3.0%; length of stay >21 days, 69.9% versus 10.7%). Young age, high complexity, previous cardiothoracic operation, preoperative length of stay more than 1 day, preoperative ventilator support, and presence of a genetic abnormality were associated with major infection after backward selection (p < 0.001). Estimated infection risk ranged from less than 0.1% to 13.3%; the model discrimination was good (c index, 0.79).
Conclusions: We created a simple bedside tool to identify children at high risk for major infection after cardiac surgery. These patients may be targeted for interventions to reduce the risk of infection and for inclusion in future clinical trials.
2010 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Major infection after pediatric cardiac surgery: external validation of risk estimation model.Ann Thorac Surg. 2012 Dec;94(6):2091-5. doi: 10.1016/j.athoracsur.2012.07.079. Epub 2012 Oct 4. Ann Thorac Surg. 2012. PMID: 23040826
-
A Study of Practice Behavior for Endotracheal Intubation Site for Children With Congenital Heart Disease Undergoing Surgery: Impact of Endotracheal Intubation Site on Perioperative Outcomes-An Analysis of the Society of Thoracic Surgeons Congenital Cardiac Anesthesia Society Database.Anesth Analg. 2019 Oct;129(4):1061-1068. doi: 10.1213/ANE.0000000000003594. Anesth Analg. 2019. PMID: 30198928
-
Delayed Sternal Closure in Infant Heart Surgery-The Importance of Where and When: An Analysis of the STS Congenital Heart Surgery Database.Ann Thorac Surg. 2016 Nov;102(5):1565-1572. doi: 10.1016/j.athoracsur.2016.08.081. Epub 2016 Oct 6. Ann Thorac Surg. 2016. PMID: 27720371
-
The Society of Thoracic Surgeons Congenital Heart Surgery Database Public Reporting Initiative.Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2017 Jan;20:43-48. doi: 10.1053/j.pcsu.2016.09.008. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2017. PMID: 28007064 Review.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
Topical negative pressure for the treatment of neonatal post-sternotomy wound dehiscence.Ann R Coll Surg Engl. 2012 Jan;94(1):e33-5. doi: 10.1308/003588412X13171221499261. Ann R Coll Surg Engl. 2012. PMID: 22524922 Free PMC article.
-
Risk factors of nosocomial infection after cardiac surgery in children with congenital heart disease.BMC Infect Dis. 2020 Jan 21;20(1):64. doi: 10.1186/s12879-020-4769-6. BMC Infect Dis. 2020. PMID: 31964345 Free PMC article.
-
Risk Factors for Healthcare-Associated Infections After Pediatric Cardiac Surgery.Pediatr Crit Care Med. 2018 Mar;19(3):237-244. doi: 10.1097/PCC.0000000000001445. Pediatr Crit Care Med. 2018. PMID: 29319633 Free PMC article.
-
Original Article--Surgical site infections following pediatric cardiac surgery in a tertiary care hospital: Rate and risk factors.J Saudi Heart Assoc. 2021 Apr 15;33(1):1-8. doi: 10.37616/2212-5043.1234. eCollection 2021. J Saudi Heart Assoc. 2021. PMID: 33880325 Free PMC article.
-
Nontyphoidal Salmonella as a Cause of Mediastinal Abscess in a Patient With Extensive Cardiac Surgery.Cureus. 2020 Aug 21;12(8):e9924. doi: 10.7759/cureus.9924. Cureus. 2020. PMID: 32968585 Free PMC article.
References
-
- Guardia Cami MT, Jordan Garcia I, Urrea Ayala M. Nosocomial infections in pediatric patients following cardiac surgery. An Pediatr (Barc) 2008;69(1):34–8. - PubMed
-
- Urrea M, et al. Prospective incidence study of nosocomial infections in a pediatric intensive care unit. Pediatr Infect Dis J. 2003;22(6):490–4. - PubMed
-
- Valera M, et al. Nosocomial infections in pediatric cardiac surgery, Italy. Infect Control Hosp Epidemiol. 2001;22(12):771–5. - PubMed
-
- Pollock EM, et al. Early nosocomial infections in pediatric cardiovascular surgery patients. Crit Care Med. 1990;18(4):378–84. - PubMed
-
- Mehta PA, et al. Risk factors for sternal wound and other infections in pediatric cardiac surgery patients. Pediatr Infect Dis J. 2000;19(10):1000–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
