

A comparison of analgesic management for emergency department patients with sickle cell disease and renal colic
- PMID: 20173433
- PMCID: PMC3677029
- DOI: 10.1097/AJP.0b013e3181bed10c
A comparison of analgesic management for emergency department patients with sickle cell disease and renal colic
Abstract
Objectives: To determine whether there is a difference in time to initial analgesic for patients with acute pain from sickle cell disease (SCD) versus renal colic (RC) and to identify factors contributing to variance in time to analgesic.
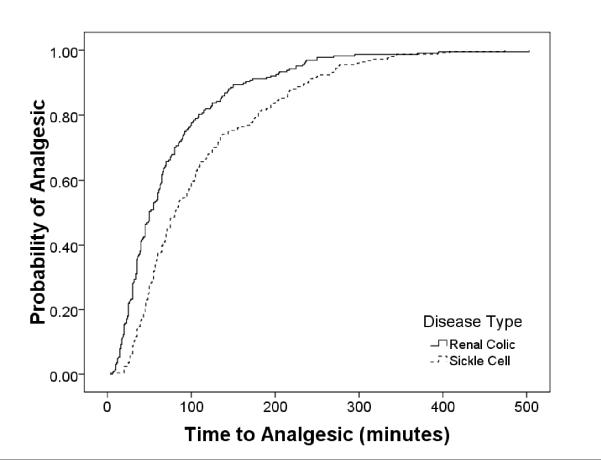
Methods: A retrospective cohort study of the adult emergency department (ED) patients with acute pain from SCD and RC in an urban ED (final ED discharge ICD-9 diagnosis codes were included). A structured medical record review abstracted the demographics, arrival shift, triage level, initial pain score, triage time, and time of initial analgesic dose. Data were compared with Kaplan-Meier plots of time to initial analgesic for both RC and SCD with the log-rank test to test for differences by disease category. A multivariable Cox regression model estimated differences in time to initial analgesic by disease category while controlling for other possible confounders.
Results: Median time to initial analgesic was 80 minutes for patients with SCD (interquartile range, 48 to 145) versus 50 minutes for patients with RC (interquartile range: 30 to 96). Patients with SCD reported a higher pain score on arrival when compared with RC patients and were more frequently assigned a higher triage priority level (P=0.05). Covariates that contributed the most delays to the model were afternoon arrival [hazard ratio (HR): 0.35, P<0.01], low acuity triage level (HR: 0.42, P<0.01), SCD diagnosis (HR: 0.61, P<0.01), and inability to obtain intravenous access (HR: 0.71, P=0.01).
Discussion: ED patients with SCD experienced longer delays in the administration of the initial analgesic compared with RC patients, despite higher arrival pain scores and triage acuity levels.
Figures
References
-
- Todd KH, Ducharme J, Choiniere M, et al. Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study. J Pain. 2007 Jun;8(6):460–466. - PubMed
-
- Pines JM, Hollander JE. Emergency department crowding is associated with poor care for patients with severe pain. Ann Emerg Med. 2008 Jan;51(1):1–5. - PubMed
-
- Mitchell R, Kelly AM, Kerr D. Does emergency department workload adversely influence timely analgesia? Emerg Med Australas. 2009 Feb;21(1):52–58. - PubMed
-
- Chu K, Brown A. Association between access block and time to parenteral opioid analgesia in renal colic: a pilot study. Emerg Med Australas. 2009 Feb;21(1):38–42. - PubMed
-
- Forero R, Mohsin M, McCarthy S, et al. Prevalence of morphine use and time to initial analgesia in an Australian emergency department. Emerg Med Australas. 2008 Apr;20(2):136–143. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
