

Nocturnal cerebral hemodynamics in snorers and in patients with obstructive sleep apnea: a near-infrared spectroscopy study
- PMID: 20175404
- PMCID: PMC2817907
- DOI: 10.1093/sleep/33.2.205
Nocturnal cerebral hemodynamics in snorers and in patients with obstructive sleep apnea: a near-infrared spectroscopy study
Abstract
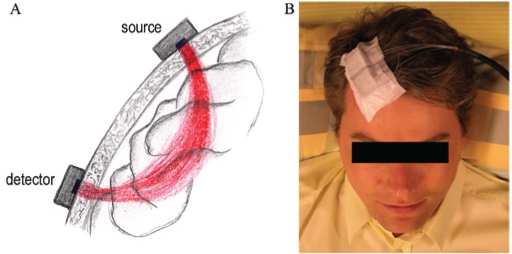
Study objectives: Sleep disordered breathing (SDB) of the obstructive type causes hemodynamic consequences, leading to an increased cerebrovascular risk. The severity of SDB at which detrimental circulatory consequences appear is matter of controversy. Aim of the present study is the investigation of cerebral hemodynamics in patients with SDB of variable severity using near-infrared spectroscopy (NIRS).
Design: N/A.
Setting: Sleep laboratory.
Patients or participants: Nineteen patients with SDB.
Interventions: N/A.
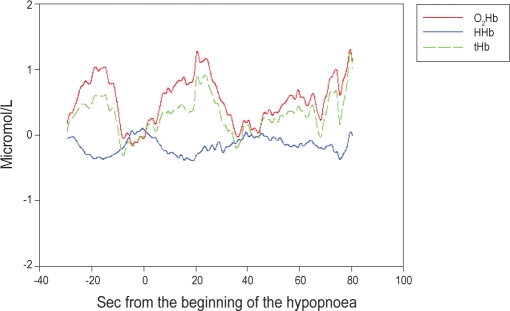
Measurements and results: Patients underwent nocturnal videopolysomnography (VPSG) coupled with cerebral NIRS. NIRS data were averaged for each patient, and a new method (integral) was applied to quantify cerebral hemodynamic alterations. Nocturnal VPSG disclosed various severities of SDB: snoring (7 patients, apnea-hypopnea index [AHI] = 2 +/- 2/h, range: 0.5-4.5); mild SDB (7 patients, AHI = 14 +/- 8/h, range: 6.3-28.6); and severe obstructive sleep apnea syndrome (5 patients, AHI = 79 +/- 20/h, range: 39.6-92.9). Relative changes of NIRS parameters were significantly larger during obstructive apneas (compared with hypopneas; mean deoxygenated hemoglobin [HHb] change of 0.72 +/- 0.23 and 0.13 +/- 0.08 micromol/L per sec, p value = 0.048) and in patients with severe SDB (as compared with patients with mild SDB and simple snorers; mean HHb change of 0.84 +/- 0.24, 0.02 +/- 0.09, and 0.2 +/- 0.08 micromol/L per sec, respectively, p value = 0.020). In this group, NIRS and concomitant changes in peripheral oxygen saturation correlated.
Conclusions: The results of this study suggest that acute cerebral hemodynamic consequences of SDB lead to a failure of autoregulatory mechanisms with brain hypoxia only in the presence of frequent apneas (AHI > 30) and obstructive events.
Figures

Comment in
-
Impaired nocturnal cerebral hemodynamics during long obstructive apneas: the key to understanding stroke in OSAS patients?Sleep. 2010 Feb;33(2):146-7. doi: 10.1093/sleep/33.2.146. Sleep. 2010. PMID: 20175397 Free PMC article. No abstract available.
Similar articles
-
Cerebral oxygenation during sleep in patients with obstructive sleep apnea: a near-infrared spectroscopy study.J Otolaryngol Head Neck Surg. 2012 Dec;41(6):437-42. J Otolaryngol Head Neck Surg. 2012. PMID: 23700590
-
How does obstructive sleep apnea alter cerebral hemodynamics?Sleep. 2023 Aug 14;46(8):zsad122. doi: 10.1093/sleep/zsad122. Sleep. 2023. PMID: 37336476 Free PMC article.
-
Noninvasive determination of brain tissue oxygenation during sleep in obstructive sleep apnea: a near-infrared spectroscopic approach.Sleep. 2007 Dec;30(12):1747-55. doi: 10.1093/sleep/30.12.1747. Sleep. 2007. PMID: 18246984 Free PMC article.
-
Insights into the effects of sleep disordered breathing on the brain in infants and children: Imaging and cerebral oxygenation measurements.Sleep Med Rev. 2020 Apr;50:101251. doi: 10.1016/j.smrv.2019.101251. Epub 2019 Dec 16. Sleep Med Rev. 2020. PMID: 31883491 Review.
-
Sleep-disordered breathing.Neurol Clin. 2012 Nov;30(4):1095-136. doi: 10.1016/j.ncl.2012.08.003. Epub 2012 Sep 15. Neurol Clin. 2012. PMID: 23099131 Review.
Cited by
-
Changes in cerebral hemoglobin indices in obstructive sleep apnea syndrome with nasal continuous positive airway pressure treatment.Sleep Breath. 2011 Sep;15(3):487-92. doi: 10.1007/s11325-010-0367-y. Epub 2010 Jun 30. Sleep Breath. 2011. PMID: 20589535
-
Best practices for fNIRS publications.Neurophotonics. 2021 Jan;8(1):012101. doi: 10.1117/1.NPh.8.1.012101. Epub 2021 Jan 7. Neurophotonics. 2021. PMID: 33442557 Free PMC article.
-
An autonomous implantable device for the prevention of death from opioid overdose.Sci Adv. 2024 Oct 25;10(43):eadr3567. doi: 10.1126/sciadv.adr3567. Epub 2024 Oct 23. Sci Adv. 2024. PMID: 39441938 Free PMC article.
-
Obstructive sleep apnea as a risk factor for cerebral white matter change in a middle-aged and older general population.Sleep. 2013 May 1;36(5):709-715B. doi: 10.5665/sleep.2632. Sleep. 2013. PMID: 23633753 Free PMC article.
-
Intracranial arterial abnormalities in patients with late onset Pompe disease (LOPD).J Inherit Metab Dis. 2016 May;39(3):391-398. doi: 10.1007/s10545-015-9913-x. Epub 2016 Feb 1. J Inherit Metab Dis. 2016. PMID: 26830551
References
-
- Diagnostic and Coding Manual. 2nd ed. Westbrook, IL: American Academy of Sleep Medicine; 2005. The International Classification of Sleep Disorders.
-
- Somers VK, Javaheri S. Cardiovascular effects of sleep-related breathing disorders. In: Kryger MH, Roth T, Dement WC, editors. Principles and practice of sleep medicine. 4th ed. Philadelphia, PA: Elsevier Inc; 2005. pp. 1180–91.
-
- Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378–1384. - PubMed
-
- Bassetti C, M Aldrich M, Chervin R, Quint D. Sleep apnea in the acute phase of TIA and stroke. Neurology. 1996;47:1167–1173. - PubMed
-
- Bassetti CL, Milanova M, Gugger M. Sleep-disordered breathing and acute ischemic stroke. Diagnosis, risk factors, treatment, evolution, and long-term clinical outcome. Stroke. 2006;37:967–972. - PubMed
