

A 12-week, randomized, double-blind, placebo-controlled study evaluating the effect of eszopiclone 2 mg on sleep/wake function in older adults with primary and comorbid insomnia
- PMID: 20175406
- PMCID: PMC2817909
- DOI: 10.1093/sleep/33.2.225
A 12-week, randomized, double-blind, placebo-controlled study evaluating the effect of eszopiclone 2 mg on sleep/wake function in older adults with primary and comorbid insomnia
Abstract
Background: Longer-term pharmacologic studies for insomnia in older individuals are sparse.
Objective: To evaluate the efficacy and safety of 12 weeks of nightly eszopiclone in elderly outpatients with insomnia.
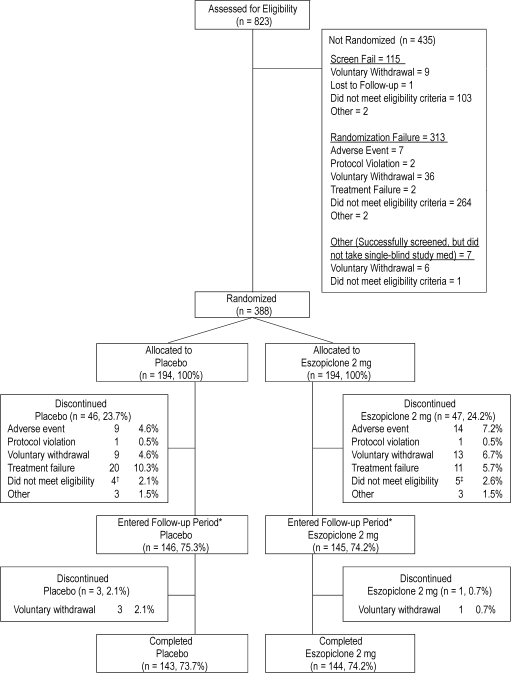
Methods: Participants (65-85 years) met DSM-IV-TR criteria for insomnia with total sleep times (TST) < or = 6 h, and wake time after sleep onset (WASO) > or = 45 min. Participants were randomized to 12 weeks of eszopiclone 2 mg (n = 194) or placebo (n = 194), followed by a 2-week single-blind placebo run-out. Subject-reported measures of sleep (sTST, sleep latency [sSL], sWASO) and daytime function (alertness, concentration, wellbeing, ability to function) were assessed. AEs were monitored.
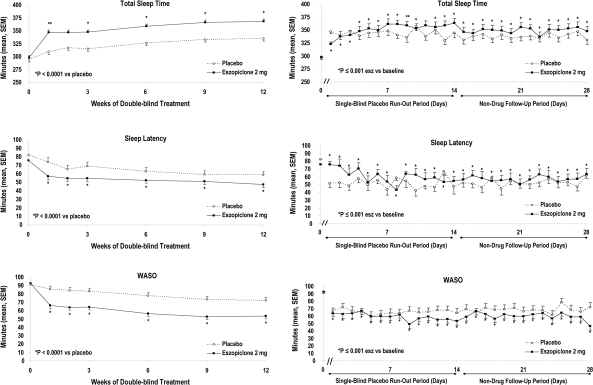
Results: Subjects treated with 2 mg eszopiclone slept longer at night on average and at every individual time point compared to baseline than placebo subjects, as measured by TST over the 12-week double-blind period (P < 0.0001). Mean sTST over the double-blind period for eszopiclone-treated subjects was 360.08 min compared to 297.86 min at baseline, a mean change of 63.24 min. Over the double-blind period, eszopiclone-treated subjects also experienced a significantly greater improvement in sSL compared to placebo, with a mean decrease of 24.62 min versus a mean decrease of 19.92 min, respectively (P = 0.0014). Eszopiclone subjects also experienced a significantly greater decrease in WASO (mean decrease of 36.4 min) compared to placebo subjects (decrease of 14.8 min) (P < 0.0001). Post-discontinuation, sleep parameters were statistically improved versus baseline for eszopiclone (P-values < or = 0.01), indicating no rebound. The most common AEs (> or = 5%) were headache (eszopiclone 13.9%, placebo 12.4%), unpleasant taste (12.4%, 1.5%), and nasopharyngitis (5.7%, 6.2%).
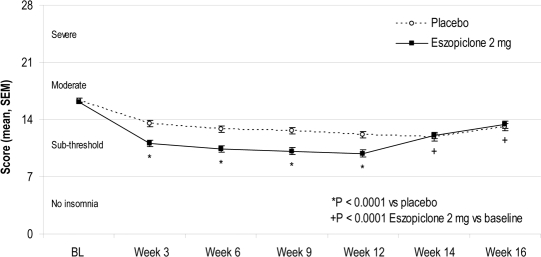
Conclusion: In this Phase IV trial of older adults with insomnia, eszopiclone significantly improved patient-reported sleep and daytime function relative to placebo. Improvements occurred within the first week and were maintained for 3 months, with no evidence of rebound insomnia following discontinuation. The 12 weeks of treatment were well tolerated.
Clinical trial information: A Long-Term Safety and Efficacy Study of Eszopiclone in Elderly Subjects With Primary Chronic Insomnia; Registration #NCT00386334; URL - http://www.clinicaltrials.gov/ct2/show/NCT00386334?term=eszopiclone&rank=24
Figures
References
-
- Ancoli-Israel S, Roth T. Characteristics of insomnia in the United States: results of the 1991 National Sleep Foundation Survey. I. Sleep. 1999;22:S347–353. - PubMed
-
- Roth T. Prevalence, associated risks, and treatment patterns of insomnia. J Clin Psychiatry. 2005;66(Suppl 9):10–13. - PubMed
-
- Mellinger GD, Balter MD, Uhlenhuth EH. Insomnia and its treatment: prevalence and correlates. Arch Gen Psychiatry. 1985;2:225–32. - PubMed
-
- Foley DJ, Monjan AA, Brown SL, Simonsick EM, Wallace RB, Blazer DG. Sleep complaints among elderly persons: an epidemiologic study of three communities. Sleep. 1995;18:425–32. - PubMed
-
- Foley DJ, Monjan A, Simonsick EM, Wallace RB, Blazer DG. Sleep Incidence and remission of insomnia among elderly adults: an epidemiologic study of 6,800 persons over three years. Sleep. 1999;22:S366–372. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
