

Assessment of out-of-field absorbed dose and equivalent dose in proton fields
- PMID: 20175494
- PMCID: PMC2803717
- DOI: 10.1118/1.3271390
Assessment of out-of-field absorbed dose and equivalent dose in proton fields
Abstract
Purpose: In proton therapy, as in other forms of radiation therapy, scattered and secondary particles produce undesired dose outside the target volume that may increase the risk of radiation-induced secondary cancer and interact with electronic devices in the treatment room. The authors implement a Monte Carlo model of this dose deposited outside passively scattered fields and compare it to measurements, determine the out-of-field equivalent dose, and estimate the change in the dose if the same target volumes were treated with an active beam scanning technique.
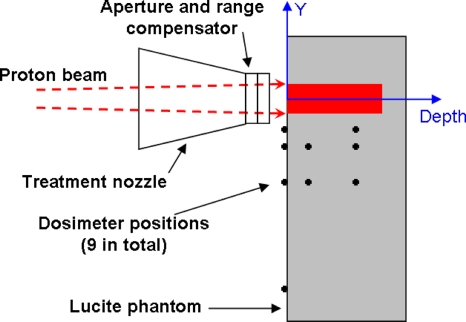
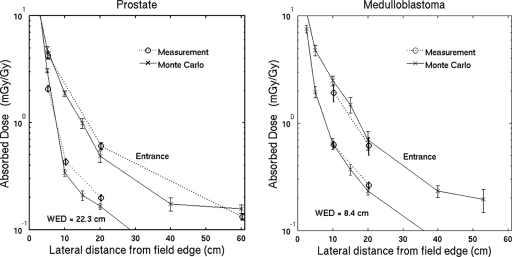
Methods: Measurements are done with a thimble ionization chamber and the Wellhofer MatriXX detector inside a Lucite phantom with field configurations based on the treatment of prostate cancer and medulloblastoma. The authors use a GEANT4 Monte Carlo simulation, demonstrated to agree well with measurements inside the primary field, to simulate fields delivered in the measurements. The partial contributions to the dose are separated in the simulation by particle type and origin.
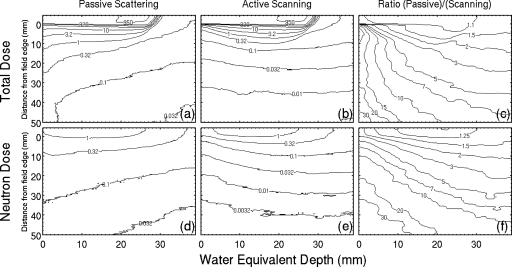
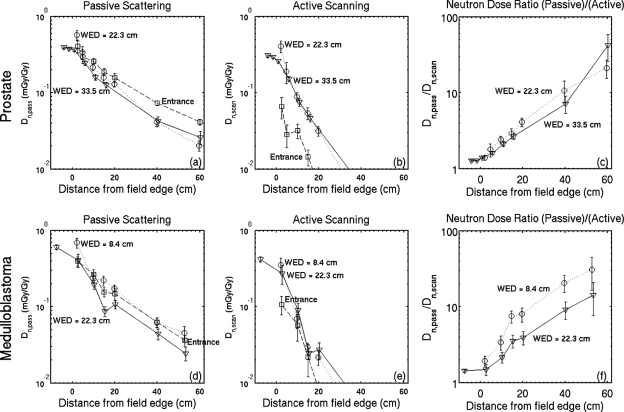
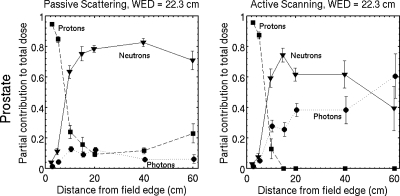
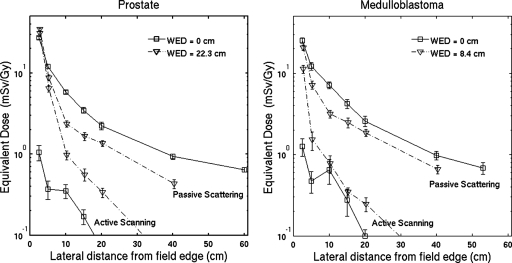
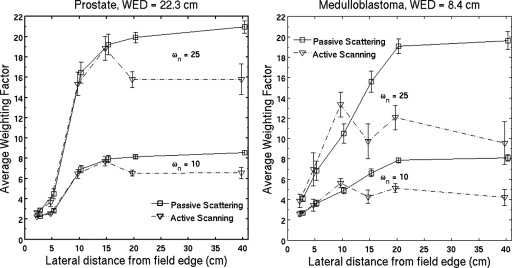
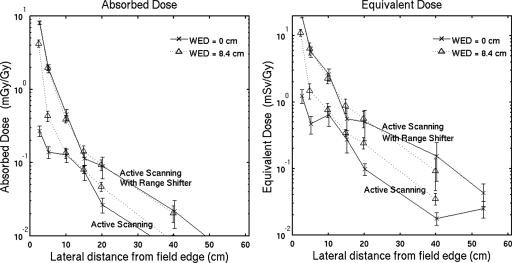
Results: The agreement between experiment and simulation in the out-of-field absorbed dose is within 30% at 10-20 cm from the field edge and 90% of the data agrees within 2 standard deviations. In passive scattering, the neutron contribution to the total dose dominates in the region downstream of the Bragg peak (65%-80% due to internally produced neutrons) and inside the phantom at distances more than 10-15 cm from the field edge. The equivalent doses using 10 for the neutron weighting factor at the entrance to the phantom and at 20 cm from the field edge are 2.2 and 2.6 mSv/Gy for the prostate cancer and cranial medulloblastoma fields, respectively. The equivalent dose at 15-20 cm from the field edge decreases with depth in passive scattering and increases with depth in active scanning. Therefore, active scanning has smaller out-of-field equivalent dose by factors of 30-45 in the entrance region and this factor decreases with depth.
Conclusions: The dose deposited immediately downstream of the primary field, in these cases, is dominated by internally produced neutrons; therefore, scattered and scanned fields may have similar risk of second cancer in this region. The authors confirm that there is a reduction in the out-of-field dose in active scanning but the effect decreases with depth. GEANT4 is suitable for simulating the dose deposited outside the primary field. The agreement with measurements is comparable to or better than the agreement reported for other implementations of Monte Carlo models. Depending on the position, the absorbed dose outside the primary field is dominated by contributions from primary protons that may or may not have scattered in the brass collimating devices. This is noteworthy as the quality factor of the low LET protons is well known and the relative dose risk in this region can thus be assessed accurately.
Figures
Similar articles
-
Validation of a Monte Carlo Framework for Out-of-Field Dose Calculations in Proton Therapy.Front Oncol. 2022 Jun 8;12:882489. doi: 10.3389/fonc.2022.882489. eCollection 2022. Front Oncol. 2022. PMID: 35756661 Free PMC article.
-
Out-of-field dose equivalents delivered by passively scattered therapeutic proton beams for clinically relevant field configurations.Int J Radiat Oncol Biol Phys. 2009 Jan 1;73(1):306-13. doi: 10.1016/j.ijrobp.2008.09.030. Int J Radiat Oncol Biol Phys. 2009. PMID: 19100924
-
A Monte Carlo-based analytic model of neutron dose equivalent for a mevion gantry-mounted passively scattered proton system for craniospinal irradiation.Med Phys. 2020 Sep;47(9):4509-4521. doi: 10.1002/mp.14299. Epub 2020 Jun 25. Med Phys. 2020. PMID: 32473612
-
Determining Out-of-Field Doses and Second Cancer Risk From Proton Therapy in Young Patients-An Overview.Front Oncol. 2022 May 31;12:892078. doi: 10.3389/fonc.2022.892078. eCollection 2022. Front Oncol. 2022. PMID: 35712488 Free PMC article. Review.
-
The Impact of Neutrons in Clinical Proton Therapy.Front Oncol. 2015 Oct 21;5:235. doi: 10.3389/fonc.2015.00235. eCollection 2015. Front Oncol. 2015. PMID: 26557501 Free PMC article. Review.
Cited by
-
Proton beam radiation therapy for prostate cancer-is the hype (and the cost) justified?Curr Urol Rep. 2013 Jun;14(3):199-208. doi: 10.1007/s11934-013-0320-2. Curr Urol Rep. 2013. PMID: 23546839 Review.
-
Monte Carlo methods for device simulations in radiation therapy.Phys Med Biol. 2021 Sep 14;66(18):10.1088/1361-6560/ac1d1f. doi: 10.1088/1361-6560/ac1d1f. Phys Med Biol. 2021. PMID: 34384063 Free PMC article. Review.
-
Assessing the Clinical Impact of Approximations in Analytical Dose Calculations for Proton Therapy.Int J Radiat Oncol Biol Phys. 2015 Aug 1;92(5):1157-1164. doi: 10.1016/j.ijrobp.2015.04.006. Epub 2015 Apr 8. Int J Radiat Oncol Biol Phys. 2015. PMID: 26025779 Free PMC article.
-
Implementation of an analytical model for leakage neutron equivalent dose in a proton radiotherapy planning system.Cancers (Basel). 2015 Mar 11;7(1):427-38. doi: 10.3390/cancers7010427. Cancers (Basel). 2015. PMID: 25768061 Free PMC article.
-
Proton therapy for early stage prostate cancer: is there a case?Onco Targets Ther. 2016 Sep 9;9:5577-86. doi: 10.2147/OTT.S108559. eCollection 2016. Onco Targets Ther. 2016. PMID: 27672328 Free PMC article. Review.
References
-
- Koehler A. M., Schneider R. J., and Sisterson J. M., “Range modulators for protons and heavy ions,” Nucl. Instrum. Methods NUIMAL 131, 437–440 (1975).10.1016/0029-554X(75)90430-9 - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
