

Identification of hypoxanthine as a urine marker for non-Hodgkin lymphoma by low-mass-ion profiling
- PMID: 20175931
- PMCID: PMC2841663
- DOI: 10.1186/1471-2407-10-55
Identification of hypoxanthine as a urine marker for non-Hodgkin lymphoma by low-mass-ion profiling
Abstract
Background: Non-Hodgkin lymphoma (NHL) is a hematologic malignancy for which good diagnostic markers are lacking. Despite continued improvement in our understanding of NHL, efforts to identify diagnostic markers have yielded dismal results. Here, we translated low-mass-ion information in urine samples from patients with NHL into a diagnostic marker.
Methods: To minimize experimental error, we tested variable parameters before MALDI-TOF analysis of low-mass ions in urine. Urine from 30 controls and 30 NHL patients was analyzed as a training set for NHL prediction. All individual peak areas were normalized to total area up to 1000 m/z. The training set analysis was repeated four times. Low-mass peaks that were not affected by changes in experimental conditions were collected using MarkerView software. Human Metabolome Database (HMDB) searches and ESI LC-MS/MS analyses were used to identify low-mass ions that exhibited differential patterns in control and NHL urines. Identified low-mass ions were validated in a blinded fashion in 95 controls and 66 NHL urines to determine their ability to discriminate NHL patients from controls.
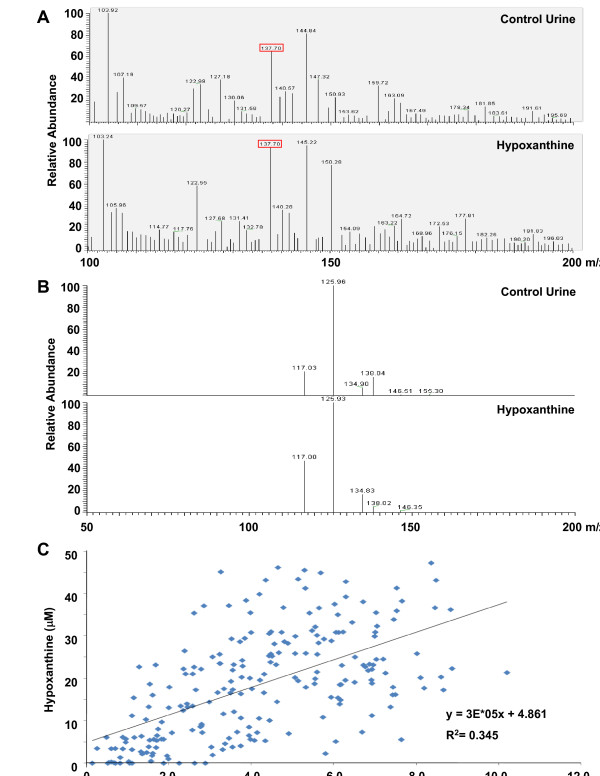
Results: The 30 highest-ranking low-mass-ion peaks were selected from the 60-urine training set, and three low-mass-ion peaks with high intensity were selected for identification. Of these, a 137.08-m/z ion showed lower mass-peak intensity in urines of NHL patients, a result that was validated in a 161-urine blind validation set (95 controls and 66 NHL urines). The 130.08-m/z ion was identified from HMDB searches and ESI LC-MS/MS analyses as hypoxanthine (HX). The HX concentration in urines of NHL patients was significantly decreased (P < 0.001) and was correlated with the mass-peak area of the 137.08-m/z ion. At an HX concentration cutoff of 17.4 microM, sensitivity and specificity were 79.2% and 78.4%, respectively.
Conclusions: The present study represents a good example of low-mass-ion profiling in the setting of disease screening using urine. This technique can be a powerful non-invasive diagnostic tool with high sensitivity and specificity for NHL screening. Furthermore, HX identified in the study may be a useful single urine marker for NHL screening.
Figures



Similar articles
-
Metabolic profiling of Escherichia coli by ion mobility-mass spectrometry with MALDI ion source.J Mass Spectrom. 2010 Dec;45(12):1383-93. doi: 10.1002/jms.1850. J Mass Spectrom. 2010. PMID: 20967735 Free PMC article.
-
Characterization of cysteinylation of pharmaceutical-grade human serum albumin by electrospray ionization mass spectrometry and low-energy collision-induced dissociation tandem mass spectrometry.Rapid Commun Mass Spectrom. 2005;19(20):2965-73. doi: 10.1002/rcm.2154. Rapid Commun Mass Spectrom. 2005. PMID: 16178042
-
[Analyzing urinary proteome patterns of metabolic syndrome patients with early renal injury by magnet bead separation and matrix-assisted laser desorption ionization time-of-flight mass spectrometry].Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2011 Oct;33(5):511-6. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2011. PMID: 22338134 Chinese.
-
Multiple ionization mass spectrometry strategy used to reveal the complexity of metabolomics.Anal Chem. 2008 Jan 15;80(2):421-9. doi: 10.1021/ac701982e. Epub 2007 Dec 18. Anal Chem. 2008. PMID: 18085752
-
Current Status of Matrix-Assisted Laser Desorption/Ionization-Time-of-Flight Mass Spectrometry (MALDI-TOF MS) in Clinical Diagnostic Microbiology.Molecules. 2020 Oct 17;25(20):4775. doi: 10.3390/molecules25204775. Molecules. 2020. PMID: 33080897 Free PMC article. Review.
Cited by
-
Identification of hypoxanthine and phosphoenolpyruvic Acid as serum markers of chemoradiotherapy response in locally advanced rectal cancer.Cancer Res Treat. 2015 Jan;47(1):78-89. doi: 10.4143/crt.2013.127. Epub 2014 Aug 21. Cancer Res Treat. 2015. PMID: 25143052 Free PMC article.
-
Specific Gut Microbiome and Serum Metabolome Changes in Lung Cancer Patients.Front Cell Infect Microbiol. 2021 Aug 30;11:725284. doi: 10.3389/fcimb.2021.725284. eCollection 2021. Front Cell Infect Microbiol. 2021. PMID: 34527604 Free PMC article.
-
Identification of Novel Serum Metabolic Biomarkers as Indicators in the Progression of Intravenous Leiomyomatosis: A High Performance Liquid Chromatography-Tandem Mass Spectrometry-Based Study.Front Cell Dev Biol. 2021 Jul 8;9:695540. doi: 10.3389/fcell.2021.695540. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34307370 Free PMC article.
-
Serum NMR metabolomics to differentiate haematologic malignancies.Oncotarget. 2018 May 11;9(36):24414-24427. doi: 10.18632/oncotarget.25311. eCollection 2018 May 11. Oncotarget. 2018. PMID: 29849950 Free PMC article.
-
Metabolomics-Based Biosignatures of Prostate Cancer in Patients Following Radiotherapy.OMICS. 2019 Apr;23(4):214-223. doi: 10.1089/omi.2019.0006. OMICS. 2019. PMID: 31009330 Free PMC article.
References
-
- Morrison VA. Non-Hodgkin's lymphoma in the elderly. Part 1: Overview and treatment of follicular lymphoma. Oncology (Williston Park) 2007;21:1104–1110. - PubMed
-
- Nicolaides C, Fountzilas G, Zoumbos N, Skarlos D, Kosmidis P, Pectasides D, Karabelis A, Giannakakis T, Symeonidis A, Papadopoulos A, Antoniou F, Pavlidis N. Diffuse large cell lymphomas: identification of prognostic factors and validation of the International Non-Hodgkin's Lymphoma Prognostic Index. A Hellenic Cooperative Oncology Group Study. Oncology. 1998;55:405–415. doi: 10.1159/000011886. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
