

Attenuated variants of Lesch-Nyhan disease
- PMID: 20176575
- PMCID: PMC2842514
- DOI: 10.1093/brain/awq013
Attenuated variants of Lesch-Nyhan disease
Abstract
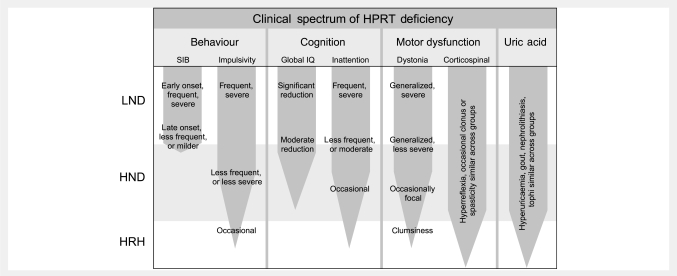
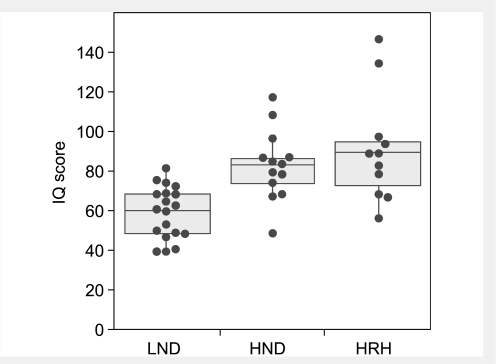
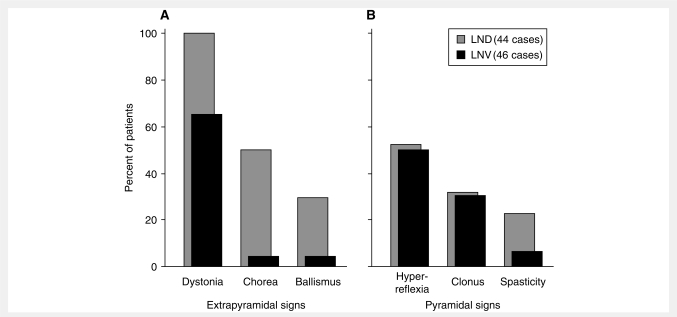
Lesch-Nyhan disease is a neurogenetic disorder caused by deficiency of the enzyme hypoxanthine-guanine phosphoribosyltransferase. The classic form of the disease is described by a characteristic syndrome that includes overproduction of uric acid, severe generalized dystonia, cognitive disability and self-injurious behaviour. In addition to the classic disease, variant forms of the disease occur wherein some clinical features are absent or unusually mild. The current studies provide the results of a prospective and multi-centre international study focusing on neurological manifestations of the largest cohort of Lesch-Nyhan disease variants evaluated to date, with 46 patients from 3 to 65 years of age coming from 34 families. All had evidence for overproduction of uric acid. Motor abnormalities were evident in 42 (91%), ranging from subtle clumsiness to severely disabling generalized dystonia. Cognitive function was affected in 31 (67%) but it was never severe. Though none exhibited self-injurious behaviours, many exhibited behaviours that were maladaptive. Only three patients had no evidence of neurological dysfunction. Our results were compared with a comprehensive review of 78 prior reports describing a total of 127 Lesch-Nyhan disease variants. Together these results define the spectrum of clinical features associated with hypoxanthine-guanine phosphoribosyltransferase deficiency. At one end of the spectrum are patients with classic Lesch-Nyhan disease and the full clinical phenotype. At the other end of the spectrum are patients with overproduction of uric acid but no apparent neurological or behavioural deficits. Inbetween are patients with varying degrees of motor, cognitive, or behavioural abnormalities. Recognition of this spectrum is valuable for understanding the pathogenesis and diagnosis of all forms of hypoxanthine-guanine phosphoribosyltransferase deficiency.
Figures
Comment in
-
Defining neurogenetic phenotypes (or how to compare needles in haystacks).Brain. 2010 Mar;133(Pt 3):649-51. doi: 10.1093/brain/awq027. Epub 2010 Feb 15. Brain. 2010. PMID: 20157007 No abstract available.
-
Attenuated variants of Lesch-Nyhan disease: the case of King James VI/I.Brain. 2010 Nov;133(11):e153; author reply e154. doi: 10.1093/brain/awq156. Epub 2010 Jul 12. Brain. 2010. PMID: 20624815 Free PMC article. No abstract available.
References
-
- Adler CH, Wrabetz L. Lesch-Nyhan variant: dystonia, ataxia, near-normal intelligence, and no self-mutilation. Mov Disord. 1996;11:583–4. - PubMed
-
- Anderson LT, Ernst M. Self-injury in Lesch-Nyhan disease. J Autism Dev Disord. 1994;24:67–81. - PubMed
-
- Anderson LT, Ernst M, Davis SV. Cognitive abilities of patients with Lesch-Nyhan disease. J Autism Dev Disord. 1992;22:189–203. - PubMed
-
- Andres A, Praga M, Ruilope LM, Martinez JM, Millet VG, Bellow I, et al. Partial deficit of hypoxanthine guanine phosphoribosyl transferase presenting as acute renal failure. Nephron. 1987;46:179–81. - PubMed
-
- Ashour R, Tintner R, Jankovic J. Striatal deformities of the hand and foot in Parkinson's; disease. Lancet Neurol. 2005;4:423–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
