

Statins for the primary prevention of cardiovascular events in women with elevated high-sensitivity C-reactive protein or dyslipidemia: results from the Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) and meta-analysis of women from primary prevention trials
- PMID: 20176986
- PMCID: PMC4439924
- DOI: 10.1161/CIRCULATIONAHA.109.906479
Statins for the primary prevention of cardiovascular events in women with elevated high-sensitivity C-reactive protein or dyslipidemia: results from the Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) and meta-analysis of women from primary prevention trials
Abstract
Background: Statin therapy in women without cardiovascular disease (CVD) is controversial, given the insufficient evidence of benefit. We analyzed sex-specific outcomes in the Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) and synthesized the results with prior trials.
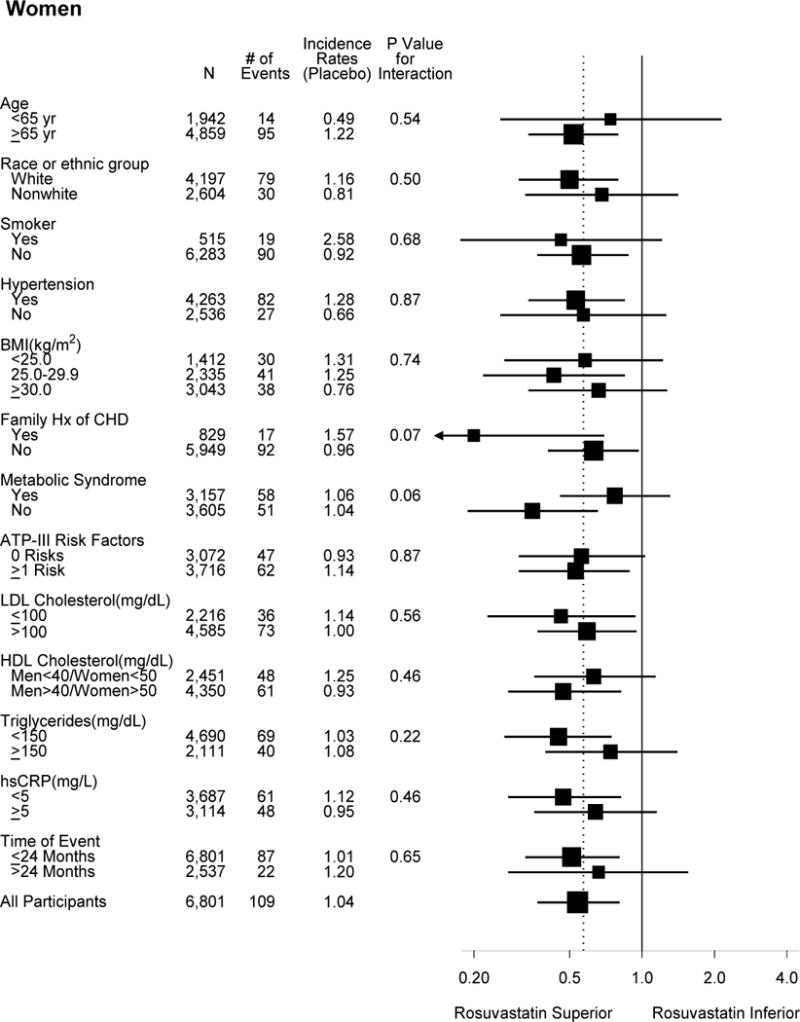
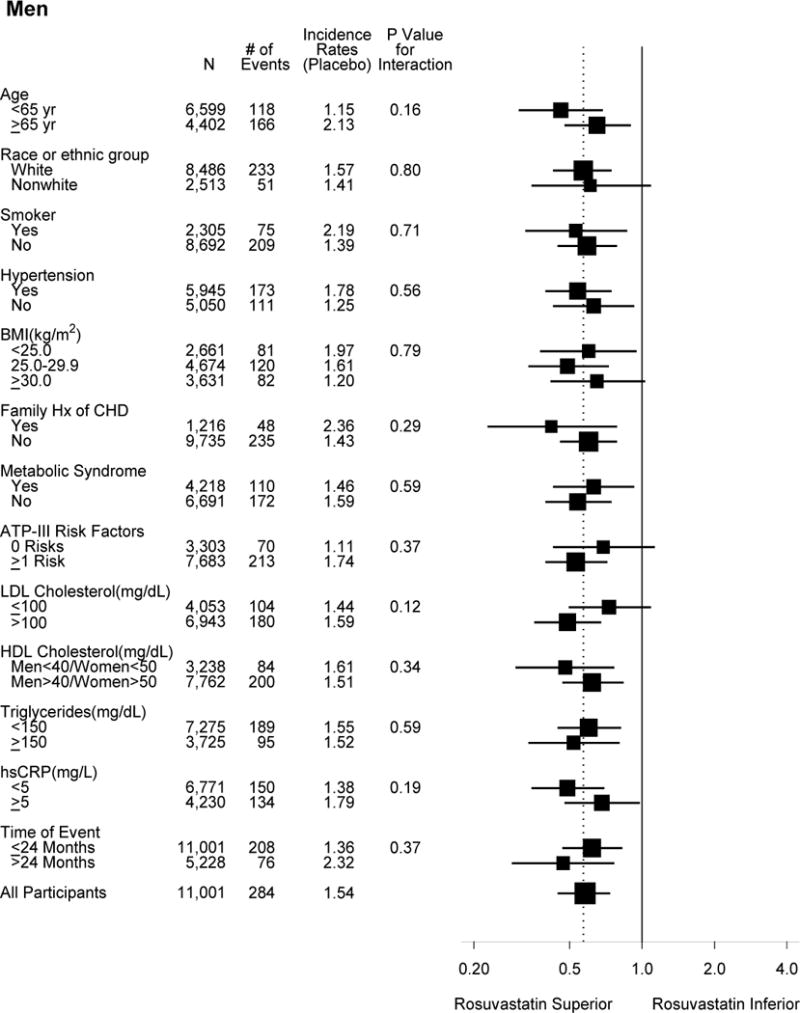
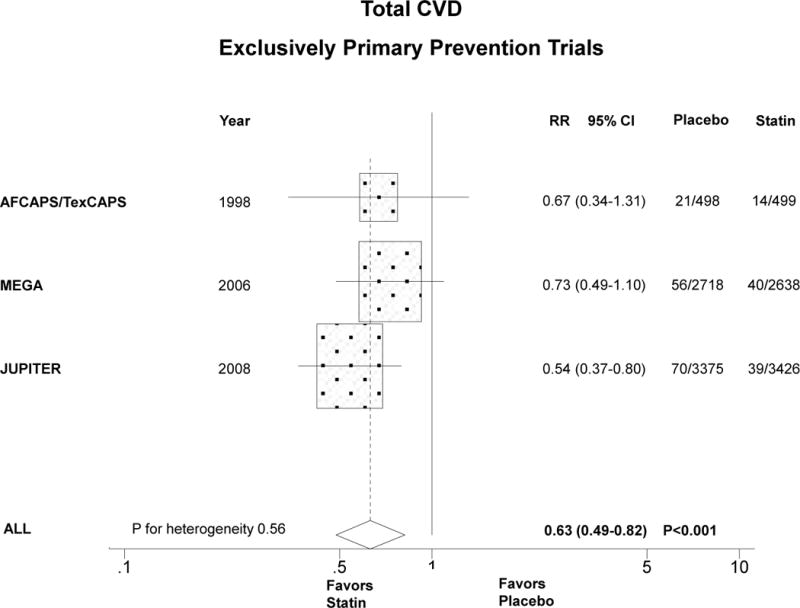
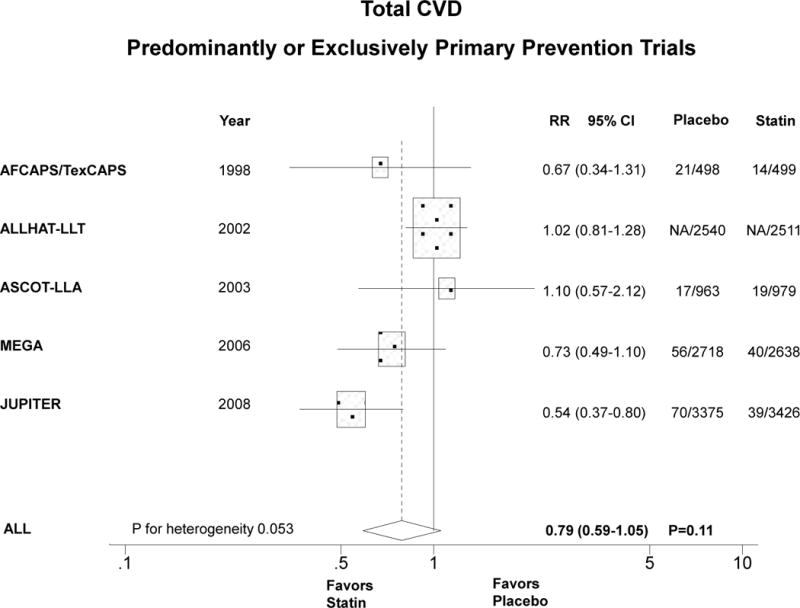
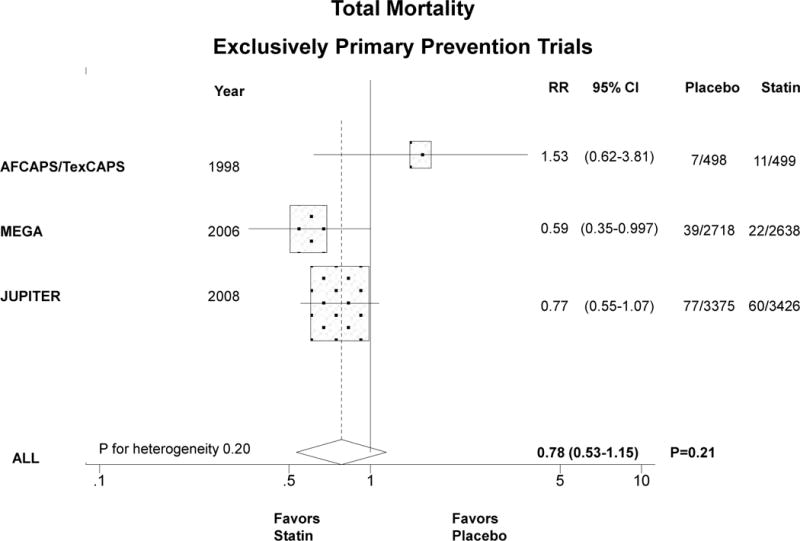
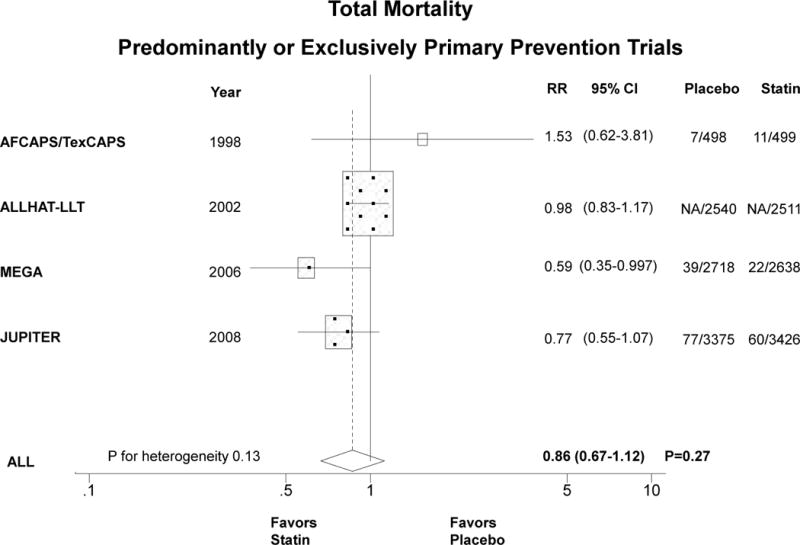
Methods and results: JUPITER participants included 6801 women > or =60 years of age and 11 001 men > or =50 years of age with high-sensitivity C-reactive protein > or =2 mg/L and low-density lipoprotein cholesterol <130 mg/dL randomized to rosuvastatin versus placebo. Meta-analysis studies were randomized placebo-controlled statin trials with predominantly or exclusively primary prevention in women and sex-specific outcomes (20 147 women; >276 CVD events; mean age, 63 to 69 years). Absolute CVD rates (per 100 person-years) in JUPITER women for rosuvastatin and placebo (0.57 and 1.04, respectively) were lower than for men (0.88 and 1.54, respectively), with similar relative risk reduction in women (hazard ratio, 0.54; 95% confidence interval, 0.37 to 0.80; P=0.002) and men (hazard ratio, 0.58; 95% confidence interval, 0.45 to 0.73; P<0.001). In women, there was significant reduction in revascularization/unstable angina and nonsignificant reductions in other components of the primary end point. Meta-analysis of 13 154 women (240 CVD events; 216 total deaths) from exclusively primary prevention trials found a significant reduction in primary CVD events with statins by a third (relative risk, 0.63; 95% confidence interval, 0.49 to 0.82; P<0.001; P for heterogeneity=0.56) with a smaller nonsignificant effect on total mortality (relative risk, 0.78; 95% confidence interval, 0.53 to 1.15; P=0.21; P for heterogeneity=0.20). Similar results were obtained for trials that were predominantly but not exclusively primary prevention.
Conclusions: JUPITER demonstrated that in primary prevention rosuvastatin reduced CVD events in women with a relative risk reduction similar to that in men, a finding supported by meta-analysis of primary prevention statin trials. Clinical Trial Registration- URL: http://www.clinicaltrials.gov. Unique identifier: NCT00239681.
Figures
Comment in
-
The numbers are in: statins for the primary prevention of cardiovascular disease in women.Circulation. 2010 Mar 9;121(9):1063-5. doi: 10.1161/CIR.0b013e3181d731c6. Epub 2010 Feb 22. Circulation. 2010. PMID: 20176993 No abstract available.
-
Rosuvastatin is similarly effective for primary prevention of cardiovascular disease in women as in men.Evid Based Med. 2010 Jun;15(3):74-5. doi: 10.1136/ebm1070. Evid Based Med. 2010. PMID: 20522679 No abstract available.
-
Letter by Wells and Eisenberg regarding article, "Statins for the primary prevention of cardiovascular events in women with elevated high-sensitivity C-reactive protein or dyslipidemia: results from the Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) and meta-analysis of women from primary prevention trials".Circulation. 2010 Dec 7;122(23):e575; author reply e577. doi: 10.1161/CIRCULATIONAHA.110.953216. Circulation. 2010. PMID: 21135368 No abstract available.
-
Letter by Vos et al regarding article, "Statins for the primary prevention of cardiovascular events in women with elevated high-sensitivity C-reactive protein or dyslipidemia: results from the Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) and meta-analysis of women from primary prevention trials".Circulation. 2010 Dec 7;122(23):e576; author reply e577. doi: 10.1161/CIRCULATIONAHA.110.954016. Circulation. 2010. PMID: 21135369 No abstract available.
References
-
- Abramson J, Wright JM. Are lipid-lowering guidelines evidence-based? Lancet. 2007;369:168–169. - PubMed
-
- Walsh JM, Pignone M. Drug treatment of hyperlipidemia in women. JAMA. 2004;291:2243–2252. - PubMed
-
- Petretta M, Costanzo P, Perrone-Filardi P, Chiariello M. Impact of gender in primary prevention of coronary heart disease with statin therapy: A meta-analysis. Int J Cardiol. 2010;138:25–31. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
