

Comanagement of hospitalized surgical patients by medicine physicians in the United States
- PMID: 20177040
- PMCID: PMC2843086
- DOI: 10.1001/archinternmed.2009.553
Comanagement of hospitalized surgical patients by medicine physicians in the United States
Abstract
Background: Comanagement of surgical patients by medicine physicians (generalist physicians or internal medicine subspecialists) has been shown to improve efficiency and to reduce adverse outcomes. We examined the extent to which comanagement is used during hospitalizations for common surgical procedures in the United States.
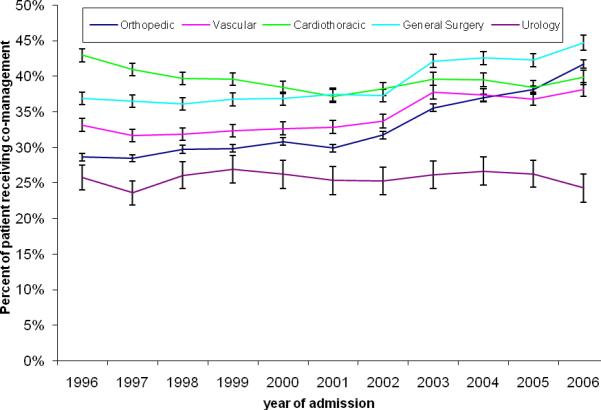
Methods: We conducted a retrospective cohort study of Medicare fee-for-service beneficiaries hospitalized for 1 of 15 inpatient surgical procedures from 1996 to 2006 (n = 694 806). We also calculated the proportion of Medicare beneficiaries comanaged by medicine physicians (generalist physicians or internal medicine subspecialists) during hospitalization. Comanagement was defined by relevant physicians (generalist or internal medicine subspecialist) submitting a claim for evaluation and management services on 70% or more of the days that the patients were hospitalized.
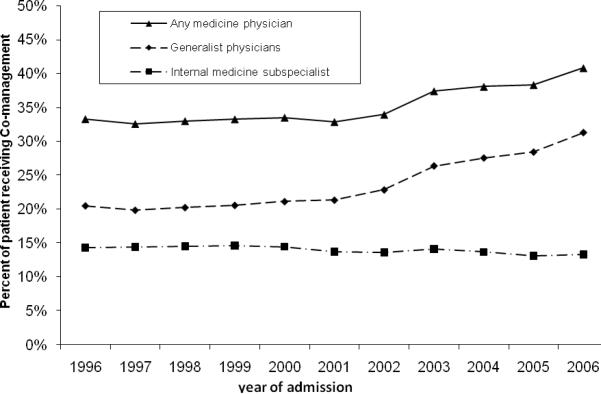
Results: Between 1996 and 2006, 35.2% of patients hospitalized for a common surgical procedure were comanaged by a medicine physician: 23.7% by a generalist physician and 14% by an internal medicine subspecialist (2.5% were comanaged by both). The percentage of patients experiencing comanagement was relatively unchanged from 1996 to 2000 and then increased sharply. The increase was entirely attributable to a surge in comanagement by generalist physicians. In a multivariable multilevel analysis, comanagement by generalist physicians increased 11.4% per year from 2001 to 2006. Patients with advanced age, with more comorbidities, or receiving care in nonteaching, midsize (200-499 beds), or for-profit hospitals were more likely to receive comanagement. All of the growth in comanagement was attributed to increased comanagement by hospitalist physicians.
Conclusions: Medical comanagement of Medicare beneficiaries hospitalized for a surgical procedure is increasing because of the increasing role of hospitalists. To meet this growing need for comanagement, training in internal medicine should include medical management of surgical patients.
Figures
Comment in
-
Engineering health in the intensive care unit.Arch Intern Med. 2010 Feb 22;170(4):319-20. doi: 10.1001/archinternmed.2009.528. Arch Intern Med. 2010. PMID: 20177033 No abstract available.
References
-
- Whinney C, Michota F. Surgical comanagement: a natural evolution of hospitalist practice. J Hosp Med. 2008 September;3(5):394–7. - PubMed
-
- Fisher AA, Davis MW, Rubenach SE, Sivakumaran S, Smith PN, Budge MM. Outcomes for older patients with hip fractures: the impact of orthopedic and geriatric medicine cocare. J Orthop Trauma. 2006 March;20(3):172–8. - PubMed
-
- Phy MP, Vanness DJ, Melton LJ, III, et al. Effects of a hospitalist model on elderly patients with hip fracture. Arch Intern Med. 2005 April 11;165(7):796–801. - PubMed
-
- Zuckerman JD, Sakales SR, Fabian DR, Frankel VH. Hip fractures in geriatric patients. Results of an interdisciplinary hospital care program. Clin Orthop Relat Res. 1992 January;(274):213–25. - PubMed
-
- Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004 July 6;141(1):28–38. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
