

The effect of multidisciplinary care teams on intensive care unit mortality
- PMID: 20177041
- PMCID: PMC4151479
- DOI: 10.1001/archinternmed.2009.521
The effect of multidisciplinary care teams on intensive care unit mortality
Erratum in
- Arch Intern Med. 2010 May 24;170(10):867. Fleisher, Lee F [corrected to Fleisher, Lee A]
Abstract
Background: Critically ill patients are medically complex and may benefit from a multidisciplinary approach to care.
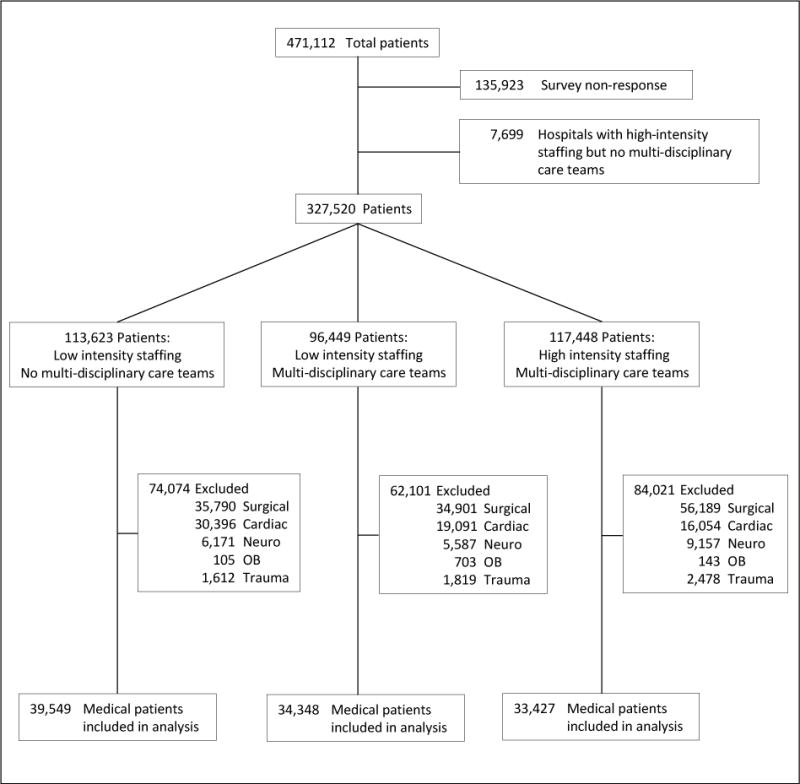
Methods: We conducted a population-based retrospective cohort study of medical patients admitted to Pennsylvania acute care hospitals (N = 169) from July 1, 2004, to June 30, 2006, linking a statewide hospital organizational survey to hospital discharge data. Multivariate logistic regression was used to determine the independent relationship between daily multidisciplinary rounds and 30-day mortality.
Results: A total of 112 hospitals and 107 324 patients were included in the final analysis. Overall 30-day mortality was 18.3%. After adjusting for patient and hospital characteristics, multidisciplinary care was associated with significant reductions in the odds of death (odds ratio [OR], 0.84; 95% confidence interval [CI], 0.76-0.93 [P = .001]). When stratifying by intensivist physician staffing, the lowest odds of death were in intensive care units (ICUs) with high-intensity physician staffing and multidisciplinary care teams (OR, 0.78; 95% CI, 0.68-0.89 [P < .001]), followed by ICUs with low-intensity physician staffing and multidisciplinary care teams (OR, 0.88; 95% CI, 0.79-0.97 [P = .01]), compared with hospitals with low-intensity physician staffing but without multidisciplinary care teams. The effects of multidisciplinary care were consistent across key subgroups including patients with sepsis, patients requiring invasive mechanical ventilation, and patients in the highest quartile of severity of illness.
Conclusions: Daily rounds by a multidisciplinary team are associated with lower mortality among medical ICU patients. The survival benefit of intensivist physician staffing is in part explained by the presence of multidisciplinary teams in high-intensity physician-staffed ICUs.
Conflict of interest statement
There are no financial conflicts of interest to disclose.
Figures
Comment in
-
Engineering health in the intensive care unit.Arch Intern Med. 2010 Feb 22;170(4):319-20. doi: 10.1001/archinternmed.2009.528. Arch Intern Med. 2010. PMID: 20177033 No abstract available.
-
Daily multidisciplinary team rounds associated with reduced 30-day mortality in medical intensive care unit patients.Evid Based Nurs. 2010 Jul;13(3):91-2. doi: 10.1136/ebn1066. Evid Based Nurs. 2010. PMID: 20584839 No abstract available.
-
The value of multidisciplinary rounds.Arch Intern Med. 2010 Jul 12;170(13):1174-5. doi: 10.1001/archinternmed.2010.214. Arch Intern Med. 2010. PMID: 20625032 No abstract available.
References
-
- Halpern NA, Pastores SM, Greenstein RJ. Critical care medicine in the United States 1985–2000: an analysis of bed numbers, use, and costs. Crit Care Med. 2004;32:1254–9. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–10. - PubMed
-
- Angus DC, Barnato AE, Linde-Zwirble WT, et al. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32:638–43. - PubMed
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353:1685–93. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
