

Continence pessary compared with behavioral therapy or combined therapy for stress incontinence: a randomized controlled trial
- PMID: 20177294
- PMCID: PMC2914312
- DOI: 10.1097/AOG.0b013e3181d055d4
Continence pessary compared with behavioral therapy or combined therapy for stress incontinence: a randomized controlled trial
Abstract
Objective: To compare the effectiveness of a continence pessary to evidence-based behavioral therapy for stress incontinence and to assess whether combined pessary and behavioral therapy is superior to single-modality therapy.
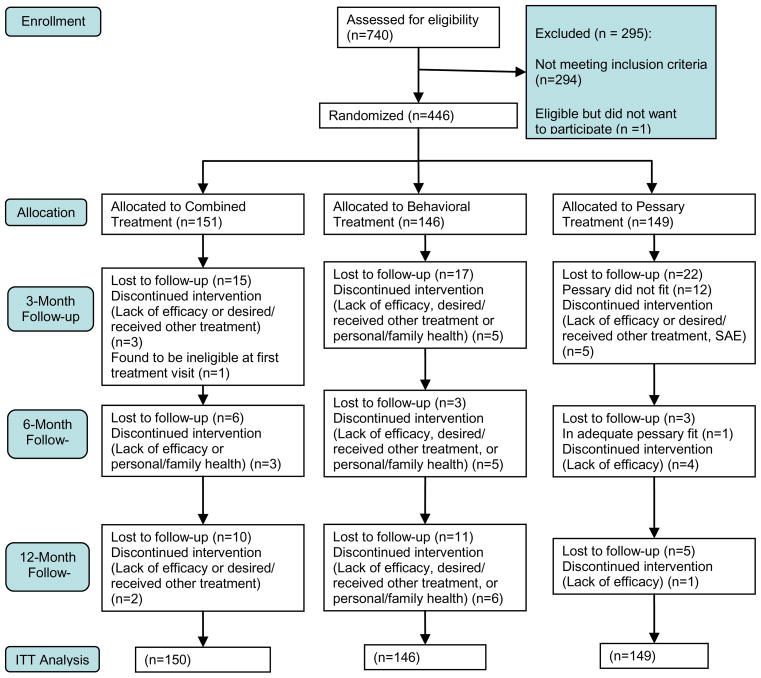
Methods: This was a multisite, randomized clinical trial (Ambulatory Treatments for Leakage Associated with Stress Incontinence [ATLAS]) that randomly assigned 446 women with stress incontinence to pessary, behavioral therapy, or combined treatment. Primary outcome measures, at 3 months, were Patient Global Impression of Improvement and the stress incontinence subscale of the Pelvic Floor Distress Inventory. A priori, to be considered clinically superior, combination therapy had to be better than both single-modality therapies. Outcome measures were repeated at 6 and 12 months. Primary analyses used an intention-to-treat approach.
Results: At 3 months, scores from 40% of the pessary group and 49% of the behavioral group were "much better" or "very much better" on the Patient Global Impression of Improvement (P=.10). Compared with the pessary group, more women in the behavioral group reported having no bothersome incontinence symptoms (49% compared with 33%, P=.006) and treatment satisfaction (75% compared with 63%, P=.02). Combination therapy was significantly better than pessary as shown on the Patient Global Impression of Improvement (53%, P=.02) and Pelvic Floor Distress Inventory (44%, P=.05) but not better than behavioral therapy; it was therefore not superior to single-modality therapy. Group differences were not sustained to 12 months on any measure, and patient satisfaction remained above 50% for all treatment groups.
Conclusion: Behavioral therapy resulted in greater patient satisfaction and fewer bothersome incontinence symptoms than pessary at 3 months, but differences did not persist to 12 months. Combination therapy was not superior to single-modality therapy.
Clinical trial registration: ClinicalTrials.gov, www.clinicaltrials.gov, NCT00270998.
References
-
- Abrams P, Cardozo L, Fall M, et al. The Standardization of terminology of lower urinary tract function: Report from the Standardization Sub-committee of the International Continence Society. Neurourol Urodynam. 2002;21:167–78. - PubMed
-
- Milsom I, Altman D, Lapitan MC, Nelson R, Sillen U, Thom D. Epidemiology of urinary (UI) and Faecal (FI) Incontinence and Pelvic Organ Prolapse. In: Abrams P, Cardozo L, Khoury S, Wein A, editors. Incontinence; 4th International Consultation on Incontinence; Paris: Health Publication Ltd; 2009. pp. 35–111.
-
- Hay-Smith J, Berghmans B, Burgio K, et al. Adult Conservative Management. In: Abrams P, Cardozo L, Khoury S, Wein A, editors. Incontinence; 4th International Consultation on Incontinence; Paris: Health Publication Ltd; 2009. pp. 1025–1120.
-
- Hay-Smith EJC, Bo K, Berghmans LCM, et al. Pelvic floor muscle training for urinary incontinence in women. Cochrane Database Syst. 2002:CD001407. Rev 1. - PubMed
-
- Shamliyan TA, Kane RL, Wyman J, Wilt TJ. Systematic review: Randomized, controlled trials of nonsurgical treatments for urinary incontinence in women. Ann Intern Med. 2008;148:459–73. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- UL1 TR000005/TR/NCATS NIH HHS/United States
- U10 HD041261/HD/NICHD NIH HHS/United States
- U01 HD041249/HD/NICHD NIH HHS/United States
- U10 HD41267/HD/NICHD NIH HHS/United States
- U10 HD054215/HD/NICHD NIH HHS/United States
- U10 HD054214/HD/NICHD NIH HHS/United States
- U10 HD54215/HD/NICHD NIH HHS/United States
- U10 HD41261/HD/NICHD NIH HHS/United States
- U10 HD54136/HD/NICHD NIH HHS/United States
- U10 HD41268/HD/NICHD NIH HHS/United States
- U10 HD041263/HD/NICHD NIH HHS/United States
- U10 HD041267/HD/NICHD NIH HHS/United States
- U10 HD054136/HD/NICHD NIH HHS/United States
- U10 HD041250/HD/NICHD NIH HHS/United States
- U10 HD41249/HD/NICHD NIH HHS/United States
- U10 HD54241/HD/NICHD NIH HHS/United States
- U10 HD 41250/HD/NICHD NIH HHS/United States
- U10 HD41248/HD/NICHD NIH HHS/United States
- U10 HD54214/HD/NICHD NIH HHS/United States
- U10 HD41263/HD/NICHD NIH HHS/United States
- UG1 HD054214/HD/NICHD NIH HHS/United States
- U10 HD041248/HD/NICHD NIH HHS/United States
- U10 HD041268/HD/NICHD NIH HHS/United States
- U10 HD054241/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
