

Risk of all-cause mortality associated with nonfatal AIDS and serious non-AIDS events among adults infected with HIV
- PMID: 20177360
- PMCID: PMC2897168
- DOI: 10.1097/QAD.0b013e3283365356
Risk of all-cause mortality associated with nonfatal AIDS and serious non-AIDS events among adults infected with HIV
Abstract
Objectives: Among patients with HIV, the risk of death associated with different AIDS events has been quantified, but the risk of death associated with non-AIDS events has not been examined. We compared the risk of all-cause mortality following AIDS versus serious non-AIDS (SNA) events in the Strategies for Management of Antiretroviral Therapy (SMART) study and the Evaluation of Subcutaneous Proleukin in a Randomized International Trial (ESPRIT).
Design: Data from 9583 HIV-infected participants, 5472 with a CD4 cell count more than 350 cells/microl enrolled in SMART and 4111 with a CD4 cell count 300 cells/microl or more enrolled in ESPRIT, were analyzed.
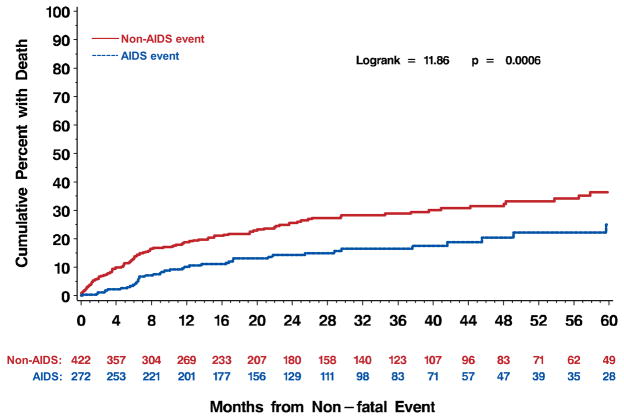
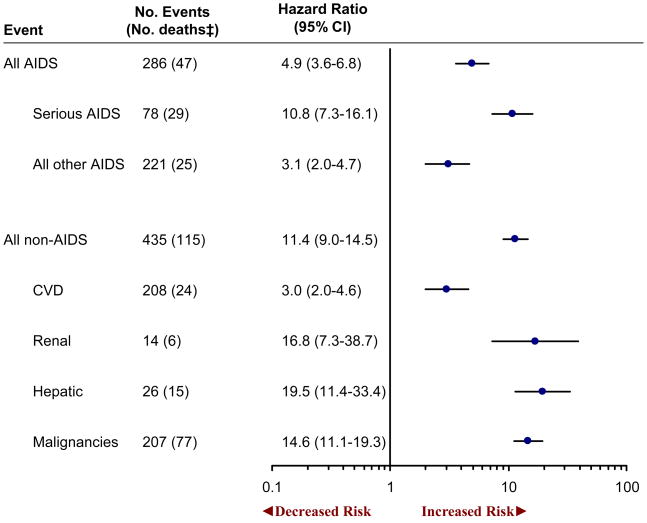
Methods: Cumulative mortality 6 months after AIDS and SNA events (cardiovascular, renal, hepatic disease, and malignancies) was estimated using the Kaplan-Meier method. Cox models were used to estimate hazard ratios associated with AIDS and SNA events on the risk of death overall and by treatment group within study.
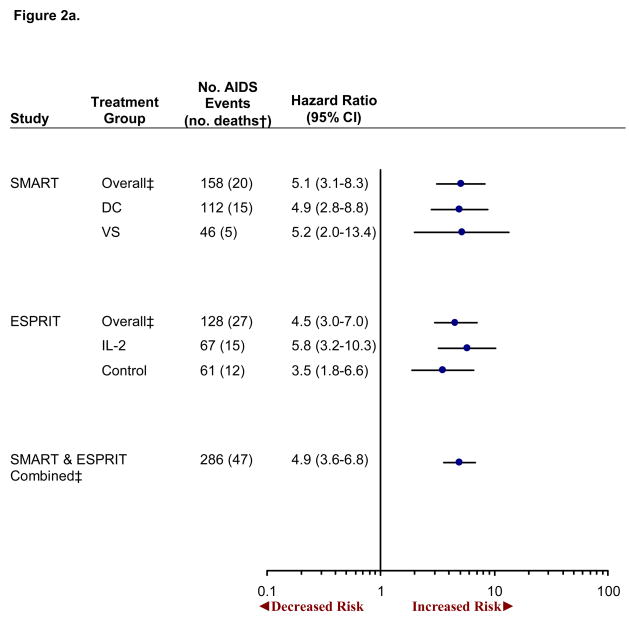
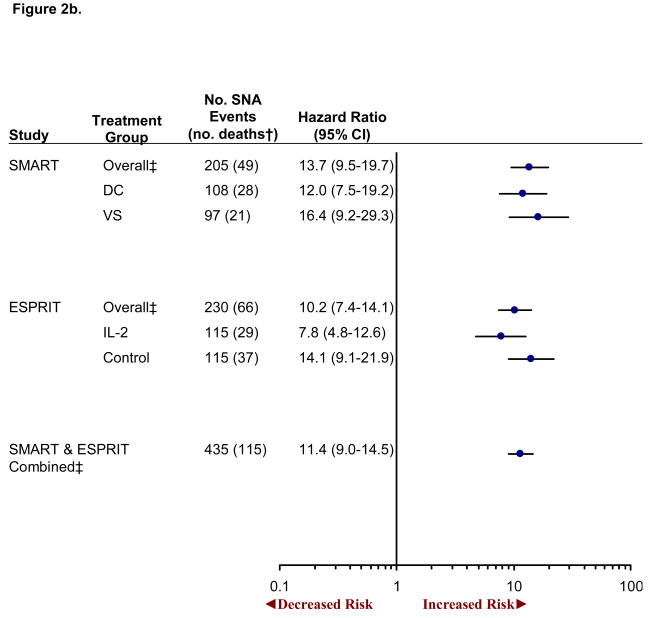
Results: AIDS and SNA events occurred in 286 and 435 participants with 47 (16%) and 115 (26%) subsequent deaths, respectively. Six-month cumulative mortality was 4.7% [95% confidence interval (CI) 2.8-8.0] after experiencing an AIDS event and 13.4% (95% CI 10.5-17.0) after experiencing an SNA event. The adjusted hazard ratio for all-cause mortality for those who experienced AIDS versus those who did not was 4.9 (95% CI 3.6-6.8). The corresponding hazard ratio for SNA was 11.4 (95% CI 9.0-14.5) (P < 0.001 for difference in hazard ratios). Findings were similar for both treatment groups in SMART and both treatment groups in ESPRIT.
Conclusion: Among HIV-infected persons with higher CD4 cell counts, SNA events occur more frequently and are associated with a greater risk of death than AIDS events. Future research should be aimed at comparing strategies to reduce morbidity and mortality associated with SNA events for HIV-infected persons.
Figures
References
-
- Mocroft A, Reiss P, Gasiorowski J, Ledergerber B, Chiesi A, Gatell J, et al. Serious Fatal and Non Fatal Non-AIDS Defining Illnesses in Europe. CROI. 2009 - PubMed
-
- Neaton JD, Grund B. Earlier initiation of antiretroviral therapy in treatment-naive patients: implications of results of treatment interruption trials. Current Opinion in HIV and AIDS. 2008;3:112–17. - PubMed
-
- Neaton JD, Wentworth DN, Rhame F, Hogan C, Abrams DI, Deyton L. Considerations in choice of a clinical endpoint for AIDS clinical trials. Stat Med. 2004;13:2107–2125. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
