

Molecular diagnostics for autosomal dominant polycystic kidney disease
- PMID: 20177400
- PMCID: PMC4050432
- DOI: 10.1038/nrneph.2010.18
Molecular diagnostics for autosomal dominant polycystic kidney disease
Abstract
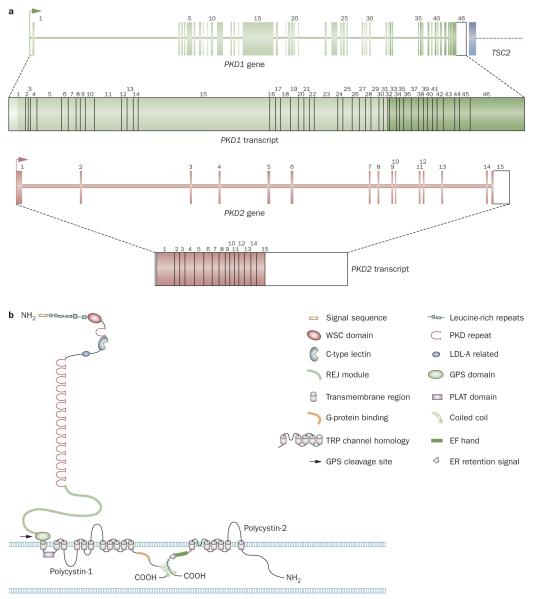
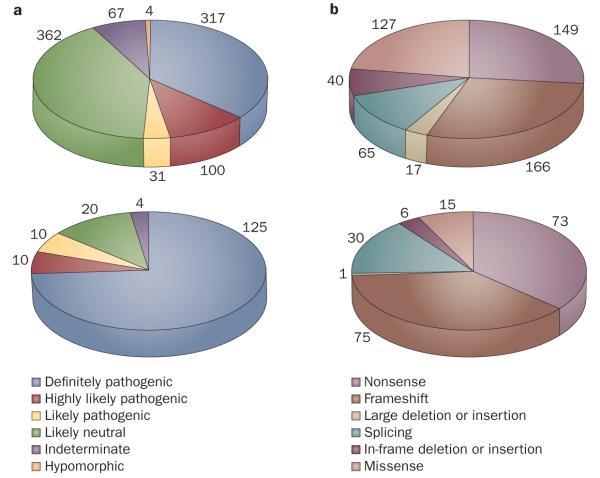
Autosomal dominant polycystic kidney disease (ADPKD) is a common nephropathy caused by mutations in either PKD1 or PKD2. Mutations in PKD1 account for approximately 85% of cases and cause more severe disease than mutations in PKD2. Diagnosis of ADPKD before the onset of symptoms is usually performed using renal imaging by either ultrasonography, CT or MRI. In general, these modalities are reliable for the diagnosis of ADPKD in older individuals. However, molecular testing can be valuable when a definite diagnosis is required in young individuals, in individuals with a negative family history of ADPKD, and to facilitate preimplantation genetic diagnosis. Although linkage-based diagnostic approaches are feasible in large families, direct mutation screening is generally more applicable. As ADPKD displays a high level of allelic heterogeneity, complete screening of both genes is required. Consequently, such screening approaches are expensive. Screening of individuals with ADPKD detects mutations in up to 91% of cases. However, only approximately 65% of patients have definite mutations with approximately 26% having nondefinite changes that require further evaluation. Collation of known variants in the ADPKD mutation database and systematic scoring of nondefinite variants is increasing the diagnostic value of molecular screening. Genic information can be of prognostic value and recent investigation of hypomorphic PKD1 alleles suggests that allelic information may also be valuable in some atypical cases. In the future, when effective therapies are developed for ADPKD, molecular testing may become increasingly widespread. Rapid developments in DNA sequencing may also revolutionize testing.
Figures
References
-
- Harris PC, Torres VE. GeneReviews at GeneTests: Medical Genetics Information Resource [database online] Copyright, University of Washginton; Seattle: 2008. 1997–2008 [online], http://www.genetests.org.
-
- Torres VE, Harris PC, Pirson Y. Autosomal dominant polycystic kidney disease. Lancet. 2007;369:1287–1301. - PubMed
-
- Dalgaard OZ. Bilateral polycystic disease of the kidneys: A follow-up of two hundred and eighty-four patients and their families. Acta Med. Scand. Suppl. 1957;328:1–255. - PubMed
-
- Iglesias CG, et al. Epidemiology of adult polycystic kidney disease, Olmsted County, Minnesota. Am. J. Kidney Dis. 1983;2:630–639. - PubMed
-
- US Renal Data System . National Institutes of Health. National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2007.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
