

Recent advances in renal phosphate handling
- PMID: 20177401
- PMCID: PMC3050486
- DOI: 10.1038/nrneph.2010.17
Recent advances in renal phosphate handling
Abstract
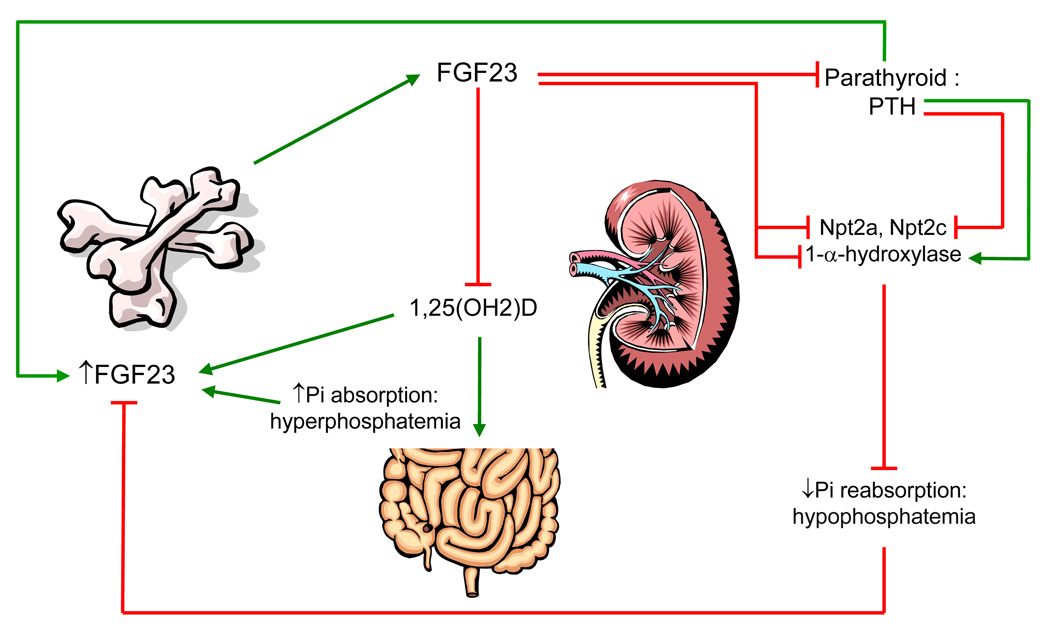
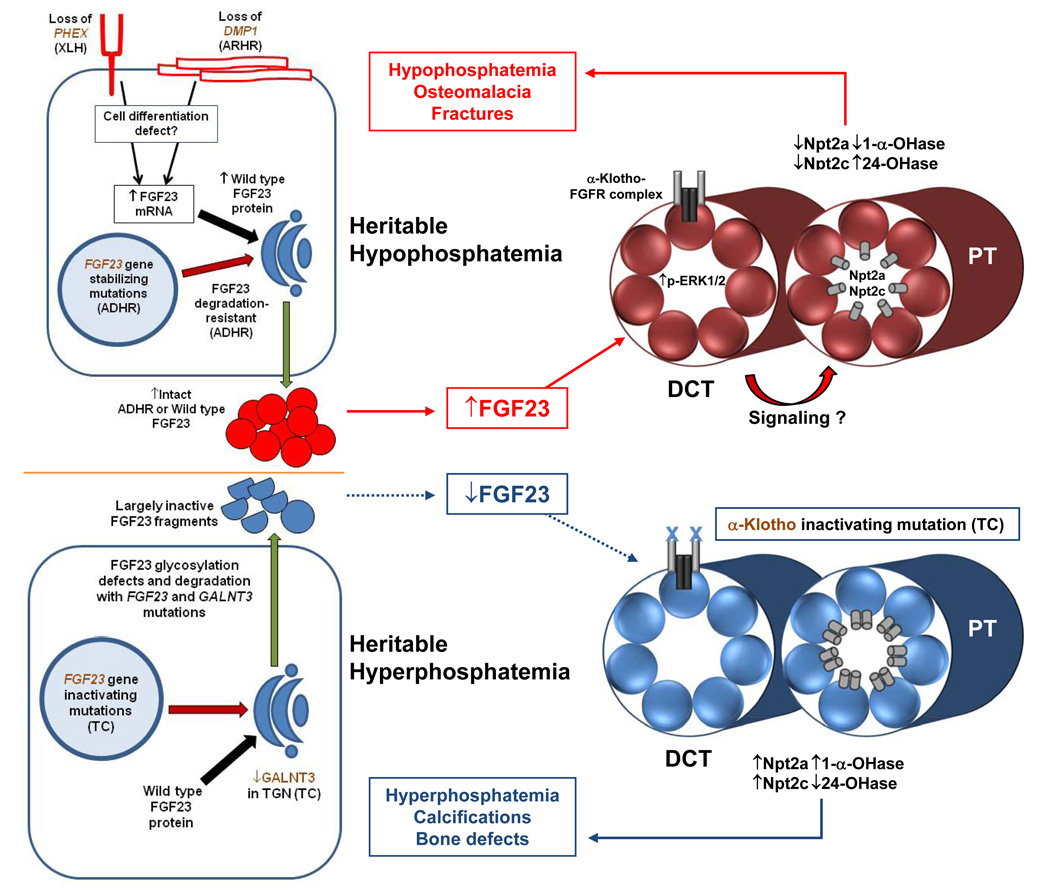
Phosphate is critical for the maintenance of skeletal integrity, is a necessary component of important biomolecules, and is central to signal transduction and cell metabolism. It is becoming clear that endocrine communication between the skeleton, kidney, and the intestine is involved in maintaining appropriate serum phosphate concentrations, and that the kidney is the primary site for minute-to-minute regulation of phosphate levels. The identification of genetic alterations in Mendelian disorders of hypophosphatemia and hyperphosphatemia has led to the isolation of novel genes and the identification of new roles for existing proteins--such as fibroblast growth factor 23 and its processing systems, the co-receptor alpha-klotho, and phosphate transporters--in the control of renal phosphate handling. Recent findings also indicate that fibroblast growth factor 23 has feedback mechanisms involving parathyroid hormone and vitamin D that control phosphate homeostasis. This Review will highlight genetic, in vitro and in vivo findings, and will discuss how these clinical and experimental discoveries have uncovered novel aspects of renal phosphate handling and opened new research and therapeutic avenues.
Figures
References
-
- Takeda E, Taketani Y, Sawada N, Sato T, Yamamoto H. The regulation and function of phosphate in the human body. Biofactors. 2004;21:345–355. - PubMed
-
- Tenenhouse HS. Regulation of phosphorus homeostasis by the type iia na/phosphate cotransporter. Annu Rev Nutr. 2005;25:197–214. - PubMed
-
- Greenberg BG, Winters RW, Graham JB. The normal range of serum inorganic phosphorus and its utility as a discriminant in the diagnosis of congenital hypophosphatemia. J Clin Endocrinol Metab. 1960;20:364–379. - PubMed
-
- Burritt MF, et al. Pediatric reference intervals for 19 biologic variables in healthy children. Mayo Clin Proc. 1990;65:329–336. - PubMed
-
- Walton J, Gray TK. Absorption of inorganic phosphate in the human small intestine. Clin Sci (Lond) 1979;56:407–412. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
