

Socioeconomic disparities in ectopic pregnancy: predictors of adverse outcomes from Illinois hospital-based care, 2000-2006
- PMID: 20177756
- PMCID: PMC2928390
- DOI: 10.1007/s10995-010-0579-6
Socioeconomic disparities in ectopic pregnancy: predictors of adverse outcomes from Illinois hospital-based care, 2000-2006
Abstract
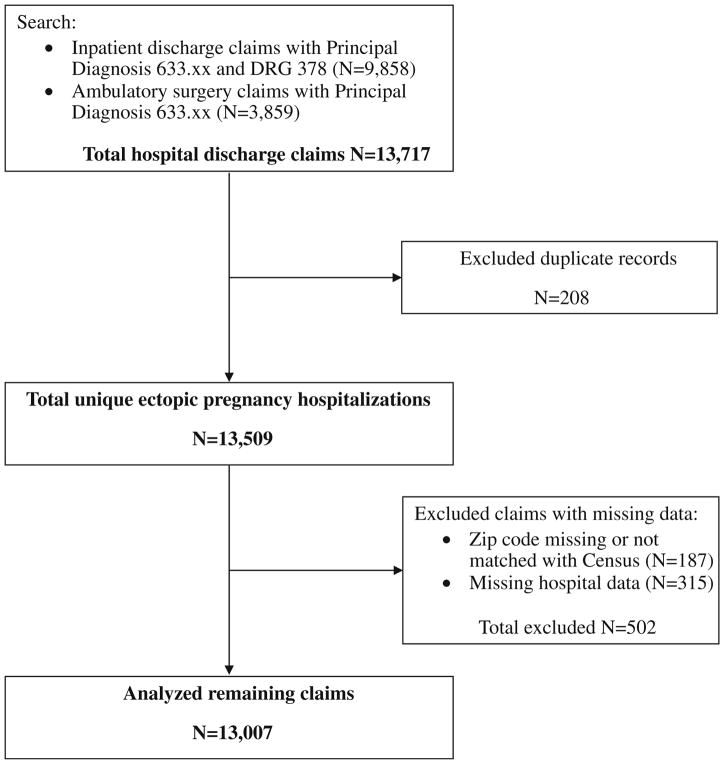
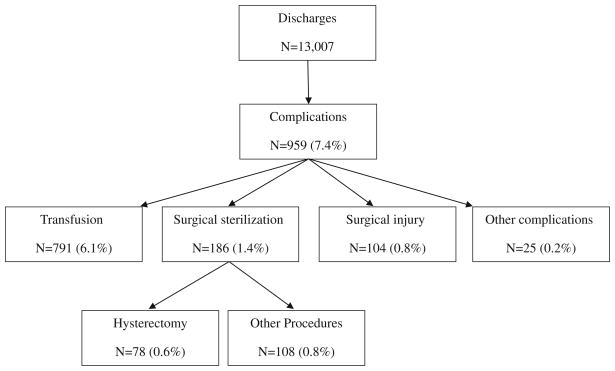
This study aimed to identify the incidence of adverse outcomes from ectopic pregnancy hospital care in Illinois (2000-2006), and assess patient, neighborhood, hospital and time factors associated with these outcomes. Discharge data from Illinois hospitals were retrospectively analyzed and ectopic pregnancies were identified using DRG and ICD-9 diagnosis codes. The primary outcome was any complication identified by ICD-9 procedure codes. Secondary outcomes were length of stay and discharge status. Residential zip codes were linked to 2000 U.S. Census data to identify patients' neighborhood demographics. Logistic regression was used to identify risk factors for adverse outcomes. Independent variables were insurance status, age, co-morbidities, neighborhood demographics, hospital type, hospital ectopic pregnancy service volume, and year of discharge. Of 13,007 ectopic pregnancy hospitalizations, 7.4% involved at least one complication identified by procedure codes. Hospitalizations covered by Medicare (for women with chronic disabilities) were more likely than those with other source or without insurance to result in surgical sterilization (OR 4.7, P = 0.012). Hospitalization longer than 2 days was more likely with Medicaid (OR 1.46, P < 0.0005) or no insurance (OR 1.35, P < 0.0005) versus other payers, and among church-operated versus secular hospitals (OR 1.21, P < 0.0005). Compared to public hospitals, private hospitals had lower rates of complications (OR 0.39, P < 0.0005) and of hospitalization longer than 2 days (OR 0.57, P < 0.0005). With time, hospitalizations became shorter (OR 0.53, P < 0.0005) and complication rates higher (OR 1.33, P = 0.024). Ectopic pregnancy patients with Medicaid, Medicare or no insurance, and those admitted to public or religious hospitals, were more likely to experience adverse outcomes.
Figures
Similar articles
-
Ectopic pregnancy morbidity and mortality in low-income women, 2004-2008.Hum Reprod. 2016 Mar;31(3):666-71. doi: 10.1093/humrep/dev332. Epub 2016 Jan 2. Hum Reprod. 2016. PMID: 26724794 Free PMC article.
-
Population-based study on the effect of socioeconomic factors and race on management and outcomes of 35,535 inpatient ectopic pregnancies.J Minim Invasive Gynecol. 2014 Sep-Oct;21(5):914-20. doi: 10.1016/j.jmig.2014.04.005. Epub 2014 Apr 24. J Minim Invasive Gynecol. 2014. PMID: 24768977
-
Pre-pregnancy and Early Prenatal Care are Associated with Lower Risk of Ectopic Pregnancy Complications in the Medicaid Population: 2004-08.Paediatr Perinat Epidemiol. 2017 Jan;31(1):4-10. doi: 10.1111/ppe.12327. Epub 2016 Nov 16. Paediatr Perinat Epidemiol. 2017. PMID: 27859439 Free PMC article.
-
Insurance status and race affect treatment and outcome of traumatic brain injury.J Surg Res. 2016 Oct;205(2):261-271. doi: 10.1016/j.jss.2016.06.087. Epub 2016 Jul 4. J Surg Res. 2016. PMID: 27664871
-
Discharge dispositions, complications, and costs of hospitalization in spinal cord tumor surgery: analysis of data from the United States Nationwide Inpatient Sample, 2003-2010.J Neurosurg Spine. 2014 Feb;20(2):125-41. doi: 10.3171/2013.9.SPINE13274. Epub 2013 Nov 29. J Neurosurg Spine. 2014. PMID: 24286530
Cited by
-
Ectopic pregnancy morbidity and mortality in low-income women, 2004-2008.Hum Reprod. 2016 Mar;31(3):666-71. doi: 10.1093/humrep/dev332. Epub 2016 Jan 2. Hum Reprod. 2016. PMID: 26724794 Free PMC article.
-
Fragmentation of Care in Ectopic Pregnancy.Matern Child Health J. 2016 May;20(5):955-61. doi: 10.1007/s10995-016-1979-z. Matern Child Health J. 2016. PMID: 26987855
-
Ectopic pregnancy rates in the Medicaid population.Am J Obstet Gynecol. 2013 Apr;208(4):274.e1-7. doi: 10.1016/j.ajog.2012.12.038. Epub 2013 Jan 8. Am J Obstet Gynecol. 2013. PMID: 23313717 Free PMC article.
-
Temporal trends in severe morbidity and mortality associated with ectopic pregnancy requiring hospitalisation in Washington State, USA: a population-based study.BMJ Open. 2019 Feb 19;9(2):e024353. doi: 10.1136/bmjopen-2018-024353. BMJ Open. 2019. PMID: 30782901 Free PMC article.
-
Awareness about a life-threatening condition: ectopic pregnancy in a network for surveillance of severe maternal morbidity in Brazil.Biomed Res Int. 2014;2014:965724. doi: 10.1155/2014/965724. Epub 2014 Mar 19. Biomed Res Int. 2014. PMID: 24772441 Free PMC article. Clinical Trial.
References
-
- Goldner TE, Lawson HW, Xia Z, Atrash HK. Surveillance for ectopic pregnancy—United States, 1970–1989. MMWR CDC surveillance summaries. 1993;42(6):73–85. - PubMed
-
- Ego A, Subtil D, Cosson M, Legoueff F, Houfflin-Debarge V, Querleu D. Survival analysis of fertility after ectopic pregnancy. Fertility and Sterility. 2001;75(3):560–566. - PubMed
-
- Seeber BE, Barnhart KT. Suspected ectopic pregnancy. Obstetrics and Gynecology. 2006;107(2 Pt 1):399–413. - PubMed
-
- Asplin BR, Rhodes KV, Levy H, Lurie N, Crain AL, Carlin BP, et al. Insurance status and access to urgent ambulatory care follow-up appointments. The Journal of the American Medical Association. 2005;294(10):1248–1254. - PubMed
-
- Anderson FW, Hogan JG, Ansbacher R. Sudden death: Ectopic pregnancy mortality. Obstetrics and Gynecology. 2004;103(6):1218–1223. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
