

Successful side-viewing endoscopic hemoclipping for Dieulafoy-like lesion at the brim of a periampullary diverticulum
- PMID: 20178576
- PMCID: PMC2837224
- DOI: 10.1186/1471-230X-10-24
Successful side-viewing endoscopic hemoclipping for Dieulafoy-like lesion at the brim of a periampullary diverticulum
Abstract
Background: Duodenal Dieulafoy's lesions are rare and only several cases were reported so far. Their characteristic appearance and location make it difficult to be diagnosed in the clinical practice. Massive bleeding often results from these lesions and can impede the accurate early treatment.
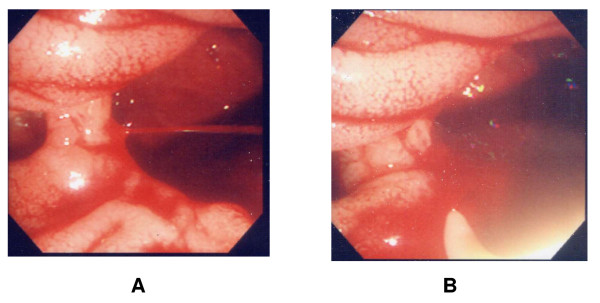
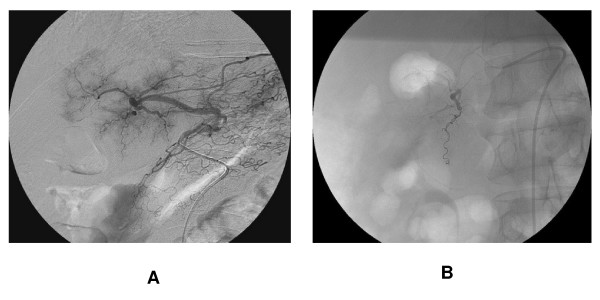
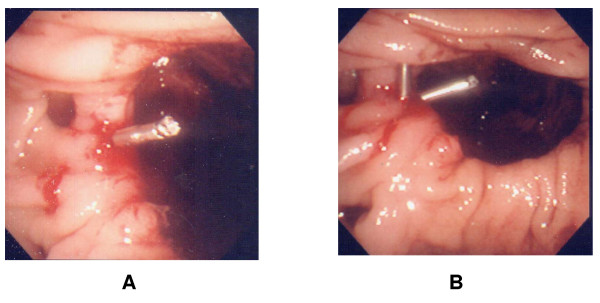
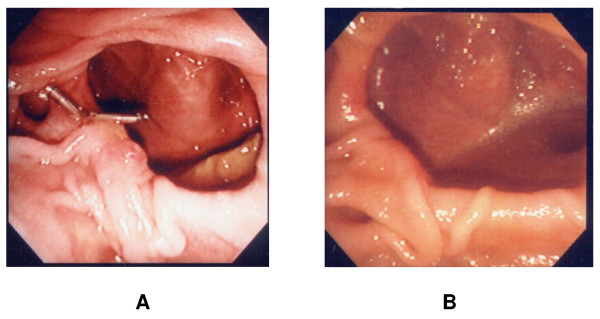
Case presentation: 67 years old male patient suffered a fatal bleeding from Dieulafoy-like lesion located at the mouth of the periampullary diverticulum. Initial endoscopic therapy and radiologic embolization failed to stop the bleeding, while direct observation and hemoclipping by the side viewing endoscopy successfully established correct diagnosis and permanent cure of the lesion.
Conclusion: Aggressive endoscopic examinations combined with the accurate endoscopic treatment should be adopted when Dieulafoy-like lesion is suspected as a possible cause of the proximal small bowel hemorrhage. Verification of the diagnosis and definitive treatment often needed repeated examination by side-viewing endoscope as well as stabilization of the patient.
Figures
Similar articles
-
[Successful Management of Periampullary Diverticular Bleeding with Hemoclipping Using Side-viewing Endoscope during Endoscopic Retrograde Cholangiopancreatography].Korean J Gastroenterol. 2016 Mar;67(3):146-9. doi: 10.4166/kjg.2016.67.3.146. Korean J Gastroenterol. 2016. PMID: 26996185 Korean.
-
Periampullary diverticulum: a case of bleeding from a periampullary diverticulum.Ann Acad Med Singap. 2005 Nov;34(10):636-8. Ann Acad Med Singap. 2005. PMID: 16382250
-
Endoscopic management and follow up of Dieulafoy lesion in the upper gastrointestinal tract.Endoscopy. 2005 May;37(5):449-53. doi: 10.1055/s-2005-861288. Endoscopy. 2005. PMID: 15844024
-
Clinical analysis and literature review of massive duodenal diverticular bleeding.World J Surg. 2001 Jul;25(7):848-55. doi: 10.1007/s00268-001-0039-y. World J Surg. 2001. PMID: 11572022 Review.
-
Massive upper gastrointestinal bleeding originating from a fourth-stage duodenal diverticulum: a case report and review of the literature.Can J Surg. 1996 Dec;39(6):510-2. Can J Surg. 1996. PMID: 8956821 Free PMC article. Review.
Cited by
-
Successful treatment of severe spontaneous periampullary bleeding with argon plasma coagulation.Clin Med Insights Gastroenterol. 2014 Aug 7;7:47-50. doi: 10.4137/CGast.S17667. eCollection 2014. Clin Med Insights Gastroenterol. 2014. PMID: 25237214 Free PMC article.
-
Fatal exulceratio simplex (dieulafoy lesion) - a case report and review.Forensic Sci Med Pathol. 2025 Jun;21(2):1030-1035. doi: 10.1007/s12024-024-00895-4. Epub 2024 Sep 19. Forensic Sci Med Pathol. 2025. PMID: 39298100 Free PMC article. Review.
-
Perforated Duodenal Diverticulum With Postoperative Diverticulum Bleeding Successfully Treated Using Transcatheter Arterial Embolization.Cureus. 2021 Sep 23;13(9):e18219. doi: 10.7759/cureus.18219. eCollection 2021 Sep. Cureus. 2021. PMID: 34722030 Free PMC article.
-
Active bleeding from a periampullary duodenal diverticulum that was difficult to diagnose but successfully treated using hemostatic forceps: a case report.J Med Case Rep. 2012 Oct 26;6:367. doi: 10.1186/1752-1947-6-367. J Med Case Rep. 2012. PMID: 23101939 Free PMC article.
-
Two Cases of Bleeding Angiodysplasias Within Duodenal Diverticulum.ACG Case Rep J. 2019 Mar 6;6(3):e00027. doi: 10.14309/crj.0000000000000027. eCollection 2019 Mar. ACG Case Rep J. 2019. PMID: 31620508 Free PMC article.
References
-
- Dy NM, Gostout CJ, Balm RK. Bleeding from the endoscopically-identified Dieulafoy lesion of the proximal small intestine and colon. Am J Gastroenterol. 1995;90:108–111. - PubMed
-
- Rajnakova A, Goh PM, Ngoi SS, Lim SG. ERCP in patients with periampullary diverticulum. Hepatogastroenterology. 2003;50:625–628. - PubMed
-
- Goldenberg SP, DeLuca VA Jr, Marignani P. Endoscopic treatment of Dieulafoy's lesion of the duodenum. Am J Gastroenterol. 1990;85:452–454. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
