

Relationship between minimal residual disease measured by multiparametric flow cytometry prior to allogeneic hematopoietic stem cell transplantation and outcome in children with acute lymphoblastic leukemia
- PMID: 20179088
- PMCID: PMC2878791
- DOI: 10.3324/haematol.2009.010843
Relationship between minimal residual disease measured by multiparametric flow cytometry prior to allogeneic hematopoietic stem cell transplantation and outcome in children with acute lymphoblastic leukemia
Abstract
Background: The presence of minimal residual disease detected by polymerase chain reaction techniques prior to allogeneic hematopoietic stem cell transplantation has proven to be an independent prognostic factor for poor outcome in children with acute lymphoblastic leukemia.
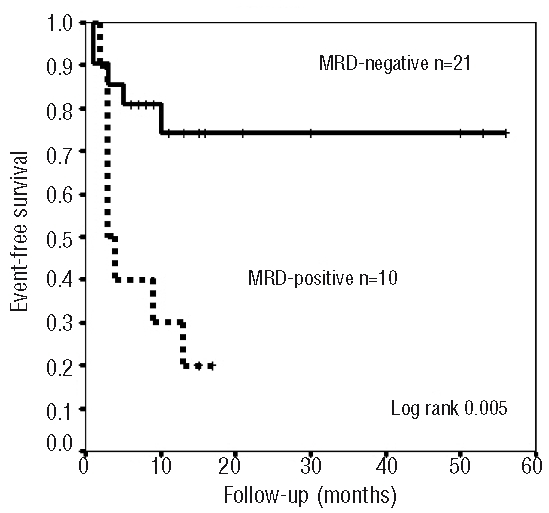
Design and methods: The aim of this study was to ascertain whether the presence of minimal residual disease detected by multiparametric flow cytometry prior to allogeneic hematopoietic stem cell transplantation is related to outcome in children acute lymphoblastic leukemia. Minimal residual disease was quantified by multiparametric flow cytometry at a median of 10 days prior to hematopoietic stem cell transplantation in 31 children (age range, 10 months to 16 years) with acute lymphoblastic leukemia. Thirteen patients were transplanted in first remission. Stem cell donors were HLA-identical siblings in 8 cases and matched unrelated donors in 23. Twenty-six children received a total body irradiation-containing conditioning regimen. According to the level of minimal residual disease, patients were divided into two groups: minimal residual disease-positive (>or=0.01%) (n=10) and minimal residual disease-negative (<0.01%) (n=21).
Results: Estimated event-free survival rates at 2 years for the minimal residual disease-negative and -positive subgroups were 74% and 20%, respectively (P=0.004) and overall survival rates were 80% and 20%, respectively (P=0.005). Bivariate analysis identified pre-transplant minimal residual disease as the only significant factor for relapse and also for death (P<0.01).
Conclusions: The presence of minimal residual disease measured by multiparametric flow cytometry identified a group of patients with a 9.5-fold higher risk of relapse and a 3.2-fold higher risk of death than those without minimal residual disease. This study supports the strong relationship between pre-transplantation minimal residual disease measured by multiparametric flow cytometry and outcome following allogeneic hematopoietic stem cell transplantation and concur with the results of previous studies using polymerase chain reaction techniques.
Figures
References
-
- Bader P, Kreyenberg H, Henze GH, Eckert C, Reising M, Willasch A, et al. Prognostic value of minimal residual disease quantification before allogeneic stem-cell transplantation in relapsed childhood acute lymphoblastic leukaemia: the ALL-REZ BFM Study Group. J Clin Oncol. 2009;27(3):377–84. - PubMed
-
- Knechtli CJ, Goulden NJ, Hancock JP, Grandage VL, Harris El, Garland RJ, et al. Minimal residual disease status before allogeneic bone marrow transplantation is an important determinant of successful outcome for children and adolescents with acute lymphoblastic leukemia. Blood. 1998;92(11):4072–9. - PubMed
-
- Krejci O, Van der Velden V, Bader P, Kreyenberg H, Goulden N, Hancock J, et al. Level of minimal residual disease prior to hematopoietic transplantation predicts prognosis in pediatric patients with acute lymphoblastic leukemia: a report of the Pre-BMT MRD study group. Bone Marrow Transplant. 2003;32(8):849–51. - PubMed
-
- Sramkova L, Muzikova K, Fronkova E, Krejci O, Sedlacek P, Formankova R, et al. Detectable minimal residual disease before allogeneic hematopoietic stem cell transplantation predicts extremely poor prognosis in children with acute lymphoblastic leukemia. Pediatr Blood Cancer. 2007;48(1):93–100. - PubMed
-
- Uzunel M, Jaksch M, Mattsson J, Ringden O. Minimal residual disease detection after allogeneic stem cell transplantation is correlated to relapse in patients with acute lymphoblastic leukaemia. Br J Haematol. 2003;122(5):788–94. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
