

Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial
- PMID: 20179283
- PMCID: PMC2918907
- DOI: 10.1001/jama.2010.158
Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial
Abstract
Context: Goal-directed resuscitation for severe sepsis and septic shock has been reported to reduce mortality when applied in the emergency department.
Objective: To test the hypothesis of noninferiority between lactate clearance and central venous oxygen saturation (ScvO2) as goals of early sepsis resuscitation.
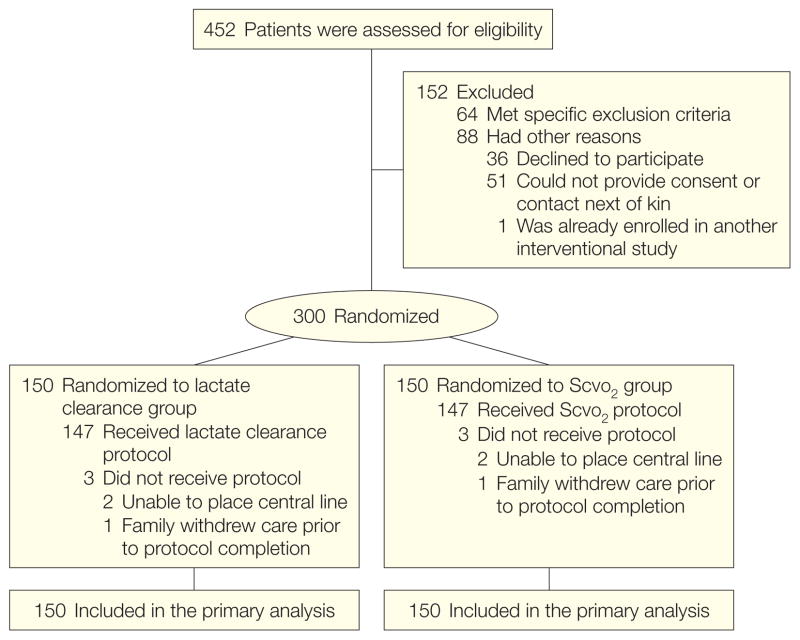
Design, setting, and patients: Multicenter randomized, noninferiority trial involving patients with severe sepsis and evidence of hypoperfusion or septic shock who were admitted to the emergency department from January 2007 to January 2009 at 1 of 3 participating US urban hospitals.
Interventions: We randomly assigned patients to 1 of 2 resuscitation protocols. The ScvO2 group was resuscitated to normalize central venous pressure, mean arterial pressure, and ScvO2 of at least 70%; and the lactate clearance group was resuscitated to normalize central venous pressure, mean arterial pressure, and lactate clearance of at least 10%. The study protocol was continued until all goals were achieved or for up to 6 hours. Clinicians who subsequently assumed the care of the patients were blinded to the treatment assignment.
Main outcome measure: The primary outcome was absolute in-hospital mortality rate; the noninferiority threshold was set at Delta equal to -10%.
Results: Of the 300 patients enrolled, 150 were assigned to each group and patients were well matched by demographic, comorbidities, and physiological features. There were no differences in treatments administered during the initial 72 hours of hospitalization. Thirty-four patients (23%) in the ScvO2 group died while in the hospital (95% confidence interval [CI], 17%-30%) compared with 25 (17%; 95% CI, 11%-24%) in the lactate clearance group. This observed difference between mortality rates did not reach the predefined -10% threshold (intent-to-treat analysis: 95% CI for the 6% difference, -3% to 15%). There were no differences in treatment-related adverse events between the groups.
Conclusion: Among patients with septic shock who were treated to normalize central venous and mean arterial pressure, additional management to normalize lactate clearance compared with management to normalize ScvO2 did not result in significantly different in-hospital mortality.
Trial registration: clinicaltrials.gov Identifier: NCT00372502.
Figures
Comment in
-
Disassembling goal-directed therapy for sepsis: a first step.JAMA. 2010 Feb 24;303(8):777-9. doi: 10.1001/jama.2010.203. JAMA. 2010. PMID: 20179290 No abstract available.
-
Lactate clearance and central venous oxygen saturation in early sepsis.JAMA. 2010 May 26;303(20):2031; author reply 2031-2. doi: 10.1001/jama.2010.658. JAMA. 2010. PMID: 20501921 No abstract available.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303–1310. - PubMed
-
- Dombrovskiy VY, Martin AA, Sunderram J, Paz HL. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003. Crit Care Med. 2007;35(5):1244–1250. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546–1554. - PubMed
-
- Wang HE, Shapiro NI, Angus DC, Yealy DM. National estimates of severe sepsis in United States emergency departments. Crit Care Med. 2007;35(8):1928–1936. - PubMed
-
- Dellinger RP, Levy MM, Carlet JM, et al. International Surviving Sepsis Campaign Guidelines Committee; American Association of Critical-Care Nurses; American College of Chest Physicians; American College of Emergency Physicians; Canadian Critical Care Society; European Society of Clinical Microbiology and Infectious Diseases; European Society of Intensive Care Medicine; European Respiratory Society; International Sepsis Forum; Japanese Association for Acute Medicine; Japanese Society of Intensive Care Medicine; Society of Critical Care Medicine; Society of Hospital Medicine; Surgical Infection Society; World Federation of Societies of Intensive and Critical Care Medicine. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36(1):296–327. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
