

Association between acute care and critical illness hospitalization and cognitive function in older adults
- PMID: 20179286
- PMCID: PMC2943865
- DOI: 10.1001/jama.2010.167
Association between acute care and critical illness hospitalization and cognitive function in older adults
Abstract
Context: Studies suggest that many survivors of critical illness experience long-term cognitive impairment but have not included premorbid measures of cognitive functioning and have not evaluated risk for dementia associated with critical illness.
Objectives: To determine whether decline in cognitive function was greater among older individuals who experienced acute care or critical illness hospitalizations relative to those not hospitalized and to determine whether the risk for incident dementia differed by these exposures.
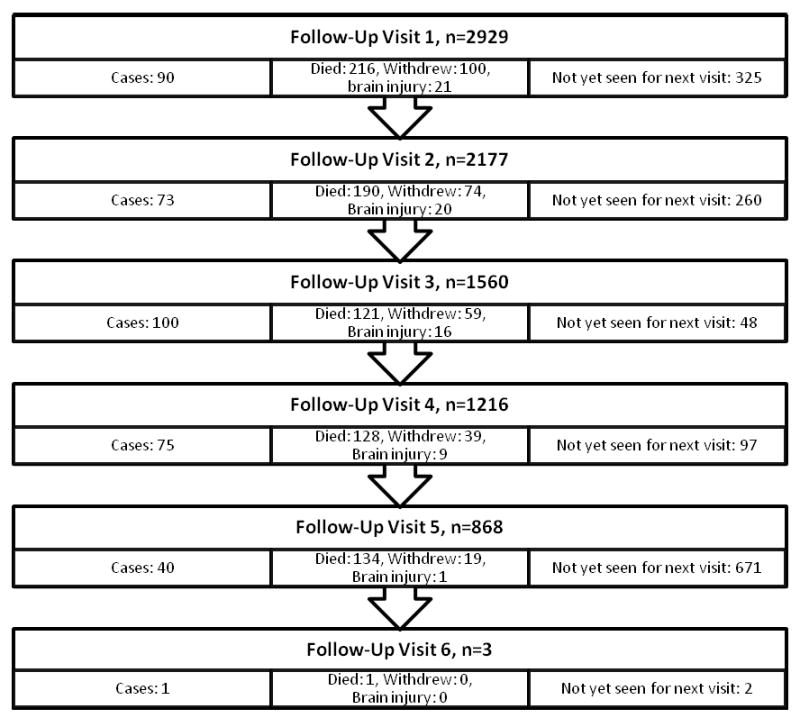
Design, setting, and participants: Analysis of data from a prospective cohort study from 1994 through 2007 comprising 2929 individuals 65 years old and older without dementia at baseline residing in the community in the Seattle area and belonging to the Group Health Cooperative. Participants with 2 or more study visits were included, and those who had a hospitalization for a diagnosis of primary brain injury were censored at the time of hospitalization. Individuals were screened with the Cognitive Abilities Screening Instrument (CASI) (score range, 0-100) every 2 years at follow-up visits, and those with a score less than 86 underwent a clinical examination for dementia.
Main outcome measures: Score on the CASI at follow-up study visits and incident dementia diagnosed in study participants, adjusted for baseline cognitive scores, age, and other risk factors.
Results: During a mean (SD) follow-up of 6.1 (3.2) years, 1601 participants had no hospitalization, 1287 had 1 or more noncritical illness hospitalizations, and 41 had 1 or more critical illness hospitalizations. The CASI score was assessed more than 45 days after discharge for 94.3% of participants. Adjusted CASI scores averaged 1.01 points lower for visits following acute care illness hospitalization compared with follow-up visits not following any hospitalization (95% confidence interval [CI], -1.33 to -0.70; P < .001) and 2.14 points lower on average for visits following critical illness hospitalization (95% CI, -4.24 to -0.03; P = .047). There were 146 cases of dementia among those not hospitalized, 228 cases of dementia among those with 1 or more noncritical illness hospitalizations, and 5 cases of dementia among those with 1 or more critical illness hospitalizations. The adjusted hazard ratio for incident dementia was 1.4 following a noncritical illness hospitalization (95% CI, 1.1 to 1.7; P = .001) and 2.3 following a critical illness hospitalization (95% CI, 0.9 to 5.7; P = .09).
Conclusions: Among a cohort of older adults without dementia at baseline, those who experienced acute care hospitalization and critical illness hospitalization had a greater likelihood of cognitive decline compared with those who had no hospitalization. Noncritical illness hospitalization was significantly associated with the development of dementia.
Comment in
-
Hospitalization and cognitive function in older adults.JAMA. 2010 Jun 2;303(21):2137-8; author reply 2138. doi: 10.1001/jama.2010.700. JAMA. 2010. PMID: 20516410 No abstract available.
References
-
- Rubenfeld GD, Herridge MS. Epidemiology and outcomes of acute lung injury. Chest. 2007 Feb;131(2):554–562. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001 Jul;29(7):1303–1310. - PubMed
-
- Carson SS, Cox CE, Holmes GM, Howard A, Carey TS. The changing epidemiology of mechanical ventilation: a population-based study. J Intensive Care Med. 2006 May-Jun;21(3):173–182. - PubMed
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005 Oct 20;353(16):1685–1693. - PubMed
-
- Herridge MS, Cheung AM, Tansey CM, et al. One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med. 2003 Feb 20;348(8):683–693. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
