

Esophageal motor disorders in terms of high-resolution esophageal pressure topography: what has changed?
- PMID: 20179690
- PMCID: PMC2888528
- DOI: 10.1038/ajg.2010.43
Esophageal motor disorders in terms of high-resolution esophageal pressure topography: what has changed?
Abstract
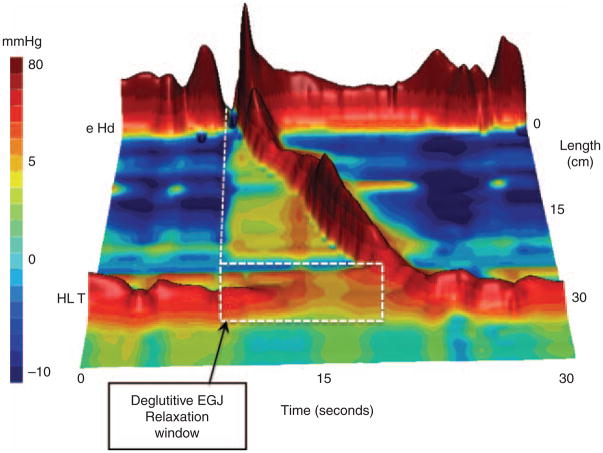
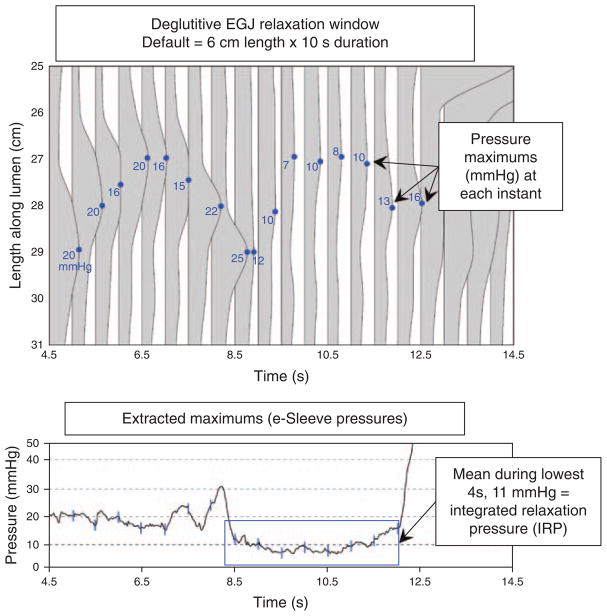
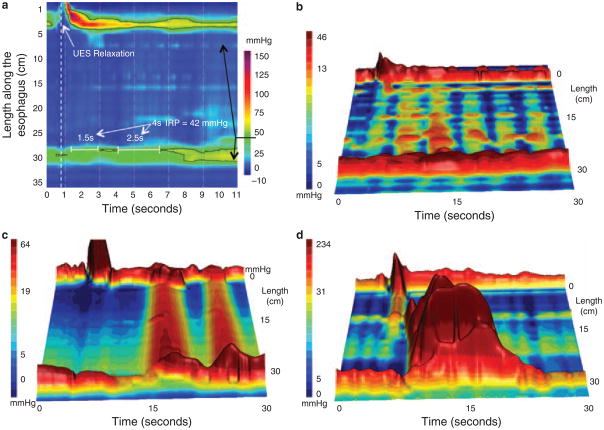
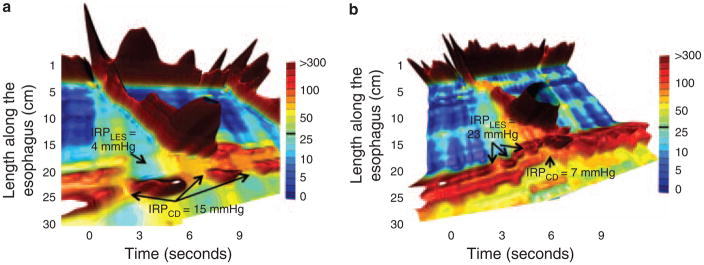
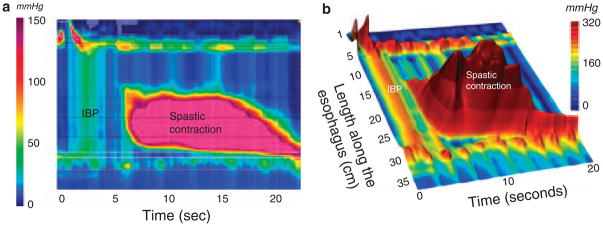
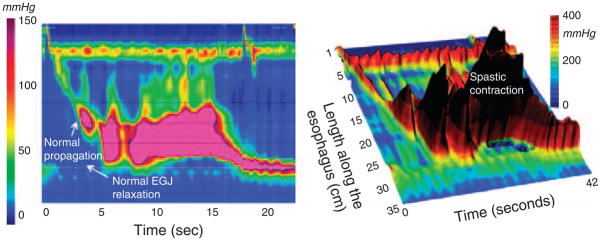
The concept of high-resolution manometry (HRM) is to use sufficient pressure sensors such that intraluminal pressure can be monitored as a continuum along luminal length much as time is viewed as a continuum in conventional manometry. When HRM is coupled with pressure topography plots, pressure amplitude is transformed into spectral colors with isobaric conditions indicated by same-colored regions on the display. Together, these technologies are called high-resolution esophageal pressure topography (HREPT). HREPT has several advantages compared with conventional manometry, the technology that it was designed to replace. (i) The contractility of the entire esophagus can be viewed simultaneously in a uniform format, (ii) standardized objective metrics can be systematically applied for interpretation, and (iii) topographic patterns of contractility are more easily recognized and have greater reproducibility than with conventional manometry. Compared with conventional manometry, HREPT has improved sensitivity for detecting achalasia, largely due to the objectivity and accuracy with which it identifies impaired esophagogastric junction (EGJ) relaxation. In addition, it has led to the subcategorization of achalasia into three clinically relevant subtypes based on the contractile function of the esophageal body: classic achalasia, achalasia with esophageal compression, and spastic achalasia. Headway has also been made in understanding hypercontractile conditions, including diffuse esophageal spasm and a newly described entity, spastic nutcracker. Ultimately, clinical experience will be the judge, but it seems likely that HREPT data, along with its well-defined functional implications, will improve the clinical management of esophageal motility disorders.
Conflict of interest statement
Figures
References
-
- Clouse RE, Staiano A. Topography of the esophageal peristaltic pressure wave. Am J Physiol. 1991;261:G677–84. - PubMed
-
- Clouse RE, Staiano A, Alrakawi A, et al. Application of topographical methods to clinical esophageal manometry. Am J Gastroenterol. 2000;95:2720–30. - PubMed
-
- Grubel C, Hiscock R, Hebbard G. Value of spatiotemporal representation of manometric data. Clin Gastroenterol Hepatol. 2008;6:525–30. - PubMed
-
- Pandolfino JE, Ghosh SK, Zhang Q, et al. Quantifying EGJ morphology and relaxation with high-resolution manometry: a study of 75 asymptomatic volunteers. Am J Physiol. 2006;290:G1033–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
