

Airway management in acute tetraplegics: a retrospective study
- PMID: 20179975
- PMCID: PMC2900019
- DOI: 10.1007/s00586-010-1328-7
Airway management in acute tetraplegics: a retrospective study
Abstract
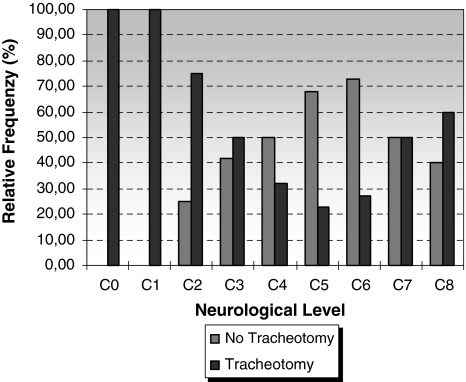
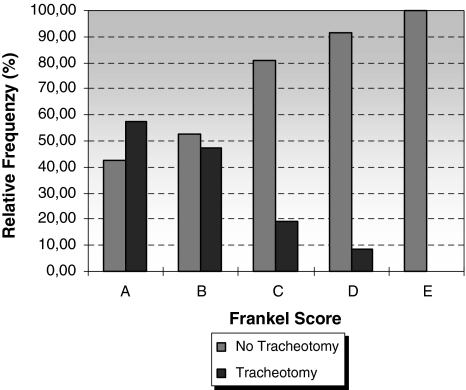
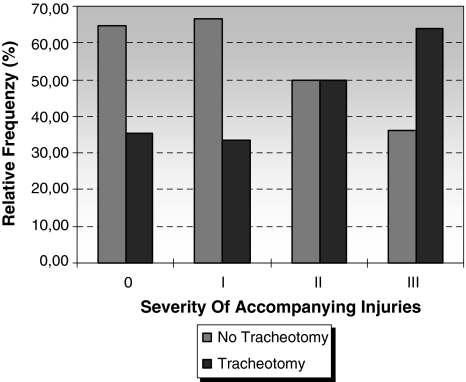
The objective of this study was to develop an evidence-based airway management protocol for patients with acute tetraplegia. The method consisted of an analysis of the medical records of patients (September 1997-December 2002) with a spinal cord injury and a neurological deficit less than 8 weeks old. Of the 175 patients, 72 (41, 14%) were tracheotomised. This was influenced by the origin of the paralysis, Frankel score, and number of cervical spine operations, accompanying injuries and accompanying illnesses. Tracheotomy did not affect the duration of treatment, duration of ventilation or length of stay in the intensive care unit. The need for a tracheotomy was able to be predicted in 73.31% with neurological level, Frankel score and severity of accompanying injuries. In patients with acute tetraplegia, primary tracheotomy is indicated in sub C1-C3 with Frankel stage A/B, sub C4-C6 with Frankel stage A/B with trauma and accompanying injuries/accompanying illnesses, and in patients with complex cervical spine trauma that requires a combined surgical approach. In other patients, an attempt at extubation should be made.
Figures
References
-
- Rodriguez JL, Steinberg SM, Luchetti FA, Gibbons KJ, Taheri PA, Flint LM. Early tracheostomy for primary airway management in the surgical critical care setting. Surgery. 1990;108:655–659. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
