

Results of the Medications at Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission
- PMID: 20180158
- PMCID: PMC2855002
- DOI: 10.1007/s11606-010-1256-6
Results of the Medications at Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission
Abstract
Background: This study was designed to determine risk factors and potential harm associated with medication errors at hospital admission.
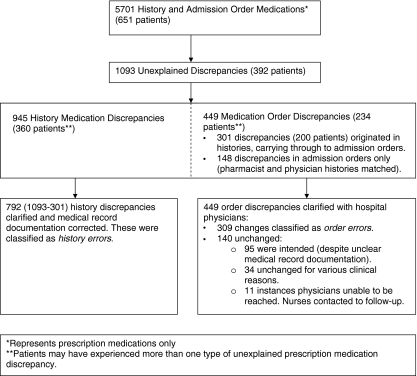
Methods: Study pharmacist and hospital-physician medication histories were compared with medication orders to identify unexplained history and order discrepancies in 651 adult medicine service inpatients with 5,701 prescription medications. Discrepancies resulting in order changes were considered errors. Logistic regression was used to analyze the association of patient demographic and clinical characteristics including patients' number of pre-admission prescription medications, pharmacies, prescribing physicians and medication changes; and presentation of medication bottles or lists. These factors were tested after controlling for patient demographics, admitting service and severity of illness.
Results: Over one-third of study patients (35.9%) experienced 309 order errors; 85% of patients had errors originate in medication histories, and almost half were omissions. Cardiovascular agents were commonly in error (29.1%). If undetected, 52.4% of order errors were rated as potentially requiring increased monitoring or intervention to preclude harm; 11.7% were rated as potentially harmful. In logistic regression analysis, patient's age > or = 65 [odds ratio (OR), 2.17; 95% confidence interval (CI), 1.09-4.30] and number of prescription medications (OR, 1.21; 95% CI, 1.14-1.29) were significantly associated with errors potentially requiring monitoring or causing harm. Presenting a medication list (OR, 0.35; 95% CI, 0.19-0.63) or bottles (OR, 0.55; 95% CI, 0.27-1.10) at admission was beneficial.
Conclusion: Over one-third of the patients in our study had a medication error at admission, and of these patients, 85% had errors originate in their medication histories. Attempts to improve the accuracy of medication histories should focus on older patients with a large number of medications. Primary care physicians and other clinicians should help patients utilize and maintain complete, accurate and understandable medication lists.
Figures
References
-
- Aspden P, Wolcott J, Bootman JL, Cronenwett LR, editors. Preventing medication errors: quality chasm series. Washington: National Academy Press; 2006.
-
- Gleason KM, Groszek JM, Sullivan C, Rooney D, Barnard C, Noskin GA. Reconciliation of discrepancies in medication histories and admission orders of newly hospitalized patients. Am J Health-Syst Pharm. 2004;61:1689–1695. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
