

Intra-operative intravenous fluid restriction reduces perioperative red blood cell transfusion in elective cardiac surgery, especially in transfusion-prone patients: a prospective, randomized controlled trial
- PMID: 20181257
- PMCID: PMC2845571
- DOI: 10.1186/1749-8090-5-7
Intra-operative intravenous fluid restriction reduces perioperative red blood cell transfusion in elective cardiac surgery, especially in transfusion-prone patients: a prospective, randomized controlled trial
Abstract
Background: Cardiac surgery is a major consumer of blood products, and hemodilution increases transfusion requirements during cardiac surgery under CPB. As intraoperative parenteral fluids contribute to hemodilution, we evaluated the hypothesis that intraoperative fluid restriction reduces packed red-cell (PRC) use, especially in transfusion-prone adults undergoing elective cardiac surgery.
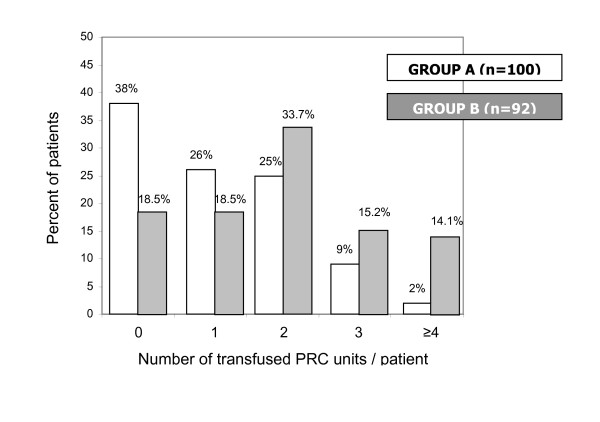
Methods: 192 patients were randomly assigned to restrictive (group A, 100 pts), or liberal (group B, 92 pts) intraoperative intravenous fluid administration. All operations were conducted by the same team (same surgeon and perfusionist). After anesthesia induction, intravenous fluids were turned off in Group A (fluid restriction) patients, who only received fluids if directed by protocol. In contrast, intravenous fluid administration was unrestricted in group B. Transfusion decisions were made by the attending anesthesiologist, based on identical transfusion guidelines for both groups.
Results: 137 of 192 patients received 289 PRC units in total. Age, sex, weight, height, BMI, BSA, LVEF, CPB duration and surgery duration did not differ between groups. Fluid balance was less positive in Group A. Fewer group A patients (62/100) required transfusion compared to group B (75/92, p < 0.04). Group A patients received fewer PRC units (113) compared to group B (176; p < 0.0001). Intraoperatively, the number of transfused units and transfused patients was lower in group A (31 u in 19 pts vs. 111 u in 62 pts; p < 0.001). Transfusions in ICU did not differ significantly between groups. Transfused patients had higher age, lower weight, height, BSA and preoperative hematocrit, but no difference in BMI or discharge hematocrit. Group B (p < 0.005) and female gender (p < 0.001) were associated with higher transfusion probability. Logistic regression identified group and preoperative hematocrit as significant predictors of transfusion.
Conclusions: Our data suggest that fluid restriction reduces intraoperative PRC transfusions without significantly increasing postoperative transfusions in cardiac surgery; this effect is more pronounced in transfusion-prone patients.
Trial registration: NCT00600704, at the United States National Institutes of Health.
Figures
Similar articles
-
The impact of fluid restriction policy in reducing the use of red blood cells in cardiac surgery.Acta Anaesthesiol Belg. 2009;60(4):221-8. Acta Anaesthesiol Belg. 2009. PMID: 20187484 Clinical Trial.
-
Influence of intraoperative fluid volume on cardiopulmonary bypass hematocrit and blood transfusions in coronary artery bypass surgery.J Extra Corpor Technol. 2008 Jun;40(2):99-108. J Extra Corpor Technol. 2008. PMID: 18705545 Free PMC article.
-
Monitoring of brain oxygen saturation (INVOS) in a protocol to direct blood transfusions during cardiac surgery: a prospective randomized clinical trial.J Cardiothorac Surg. 2013 Jun 7;8:145. doi: 10.1186/1749-8090-8-145. J Cardiothorac Surg. 2013. PMID: 23758929 Free PMC article. Clinical Trial.
-
A model for predicting transfusion requirements in head and neck surgery.Laryngoscope. 1995 Aug;105(8 Pt 2 Suppl 73):1-17. doi: 10.1288/00005537-199508001-00001. Laryngoscope. 1995. PMID: 7630307 Review.
-
Management of intraoperative fluid balance and blood conservation techniques in adult cardiac surgery.Heart Surg Forum. 2011 Feb;14(1):E28-39. doi: 10.1532/HSF98.2010111. Heart Surg Forum. 2011. PMID: 21345774 Review.
Cited by
-
Perioperative acute kidney injury.Perioper Med (Lond). 2012 Jul 4;1:6. doi: 10.1186/2047-0525-1-6. eCollection 2012. Perioper Med (Lond). 2012. PMID: 24764522 Free PMC article. Review.
-
A retrospective study from a single center of 252 patients who underwent elective pancreaticoduodenectomy to compare perioperative hemodynamic optimization therapy and usual protocols in terms of perioperative cardiac function.Exp Ther Med. 2022 Sep 28;24(5):696. doi: 10.3892/etm.2022.11632. eCollection 2022 Nov. Exp Ther Med. 2022. PMID: 36277165 Free PMC article.
-
2024 EACTS/EACTAIC Guidelines on patient blood management in adult cardiac surgery in collaboration with EBCP.Eur J Cardiothorac Surg. 2025 May 6;67(5):ezae352. doi: 10.1093/ejcts/ezae352. Eur J Cardiothorac Surg. 2025. PMID: 39385500 Free PMC article. No abstract available.
-
The effect of retrograde autologous priming volume on haemodilution and transfusion requirements during cardiac surgery.Interact Cardiovasc Thorac Surg. 2013 Jun;16(6):778-83. doi: 10.1093/icvts/ivt085. Epub 2013 Mar 12. Interact Cardiovasc Thorac Surg. 2013. PMID: 23482374 Free PMC article.
-
Factors in perioperative care that determine blood loss in liver surgery.HPB (Oxford). 2012 Apr;14(4):236-41. doi: 10.1111/j.1477-2574.2011.00433.x. Epub 2012 Feb 28. HPB (Oxford). 2012. PMID: 22404261 Free PMC article.
References
-
- Oliver E, Carrio ML, Rodriguez-Castro D, Javierre C, Farrero E, Torrado H, Castells E, Ventura JL. Relationships among haemoglobin level, packed red cell transfusion and clinical outcomes in patients after cardiac surgery. Intensive Care Med. 2009;35:1548–1555. doi: 10.1007/s00134-009-1526-0. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
